
Handling PDF files online is certainly a breeze with our PDF tool. You can fill out ks ccl medical search here in a matter of minutes. The tool is continually upgraded by our staff, getting awesome features and becoming greater. To get the process started, go through these easy steps:
Step 1: Simply hit the "Get Form Button" above on this site to get into our pdf form editor. This way, you will find everything that is necessary to work with your document.
Step 2: With this online PDF tool, you could accomplish more than just fill in blank form fields. Try all the features and make your forms seem high-quality with custom textual content added, or tweak the original input to perfection - all that comes along with an ability to insert any type of photos and sign the PDF off.
This form requires specific data to be entered, hence you should definitely take some time to fill in precisely what is required:
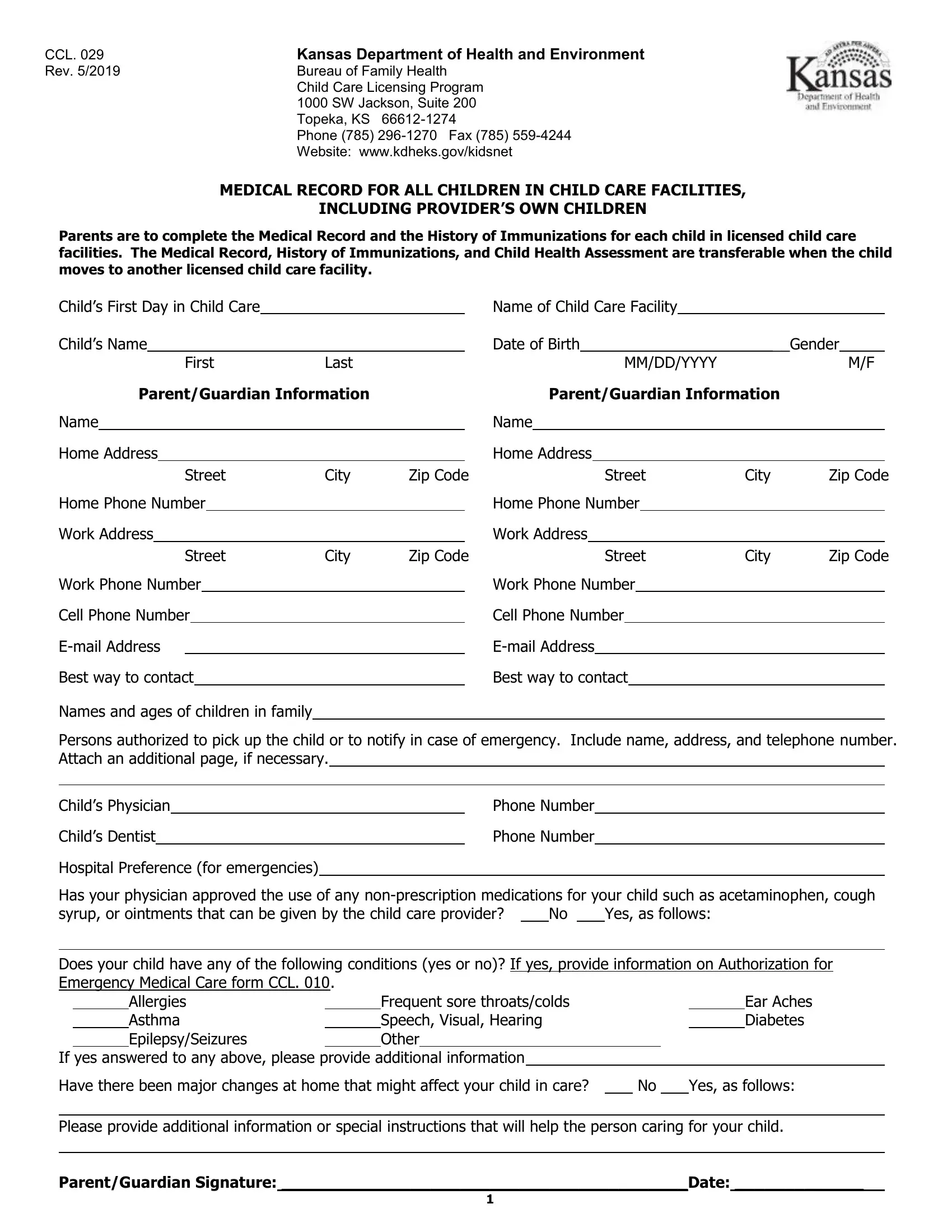
1. You should complete the ks ccl medical search correctly, therefore be attentive when filling in the sections including all these fields:
2. Once your current task is complete, take the next step – fill out all of these fields - Best way to contact Names and ages, Best way to contact, Persons authorized to pick up the, Phone Number, Phone Number, Hospital Preference for emergencies, Has your physician approved the, Yes as follows, Does your child have any of the, Allergies Asthma EpilepsySeizures, If yes answered to any above, Frequent sore throatscolds Speech, Ear Aches Diabetes, Have there been major changes at, and Yes as follows with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
3. Your next step will be simple - fill in every one of the empty fields in Have there been major changes at, and Yes as follows in order to finish this process.

4. All set to fill out the next portion! Here you'll have all these Childs Name, First, Section I For a recommended, MMDDYYYY, Date of Birth, Last, Vaccine, Record the Month Day and Year that, Diphtheria Tetanus Pertussis, DTaP, Poliomyelitis IPVOPV, Measles Mumps Rubella MMR, Hepatitis B HepB, Varicella VAR, and Hemophilus Influenzae Type B Hib empty form fields to do.
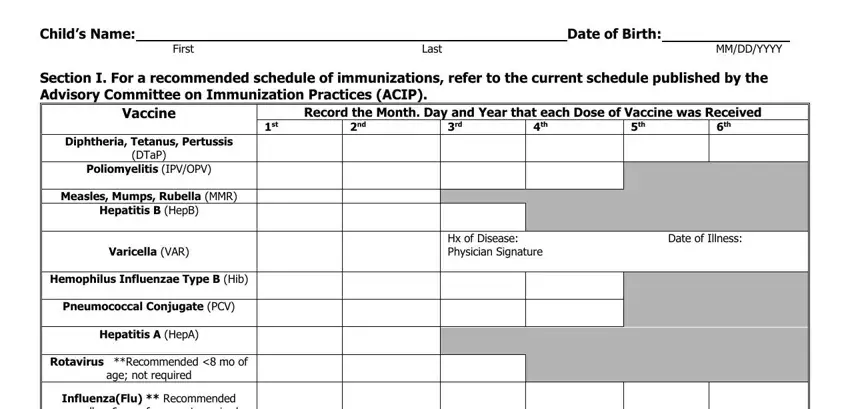
5. To finish your document, this last part includes several additional blank fields. Filling in Section II Complete this section, The following two options are the, PCV Varicella Other, Physicians Signature required Date, Section III, and ParentGuardian Signature Date is going to wrap up the process and you'll surely be done in no time!
Be extremely mindful when completing Section III and PCV Varicella Other, because this is where a lot of people make a few mistakes.
Step 3: Immediately after double-checking the filled out blanks, hit "Done" and you are good to go! Download the ks ccl medical search when you register at FormsPal for a free trial. Readily view the pdf form from your FormsPal account, along with any modifications and adjustments being all kept! FormsPal ensures your data privacy via a protected system that never saves or distributes any personal data involved. Rest assured knowing your files are kept protected each time you work with our service!