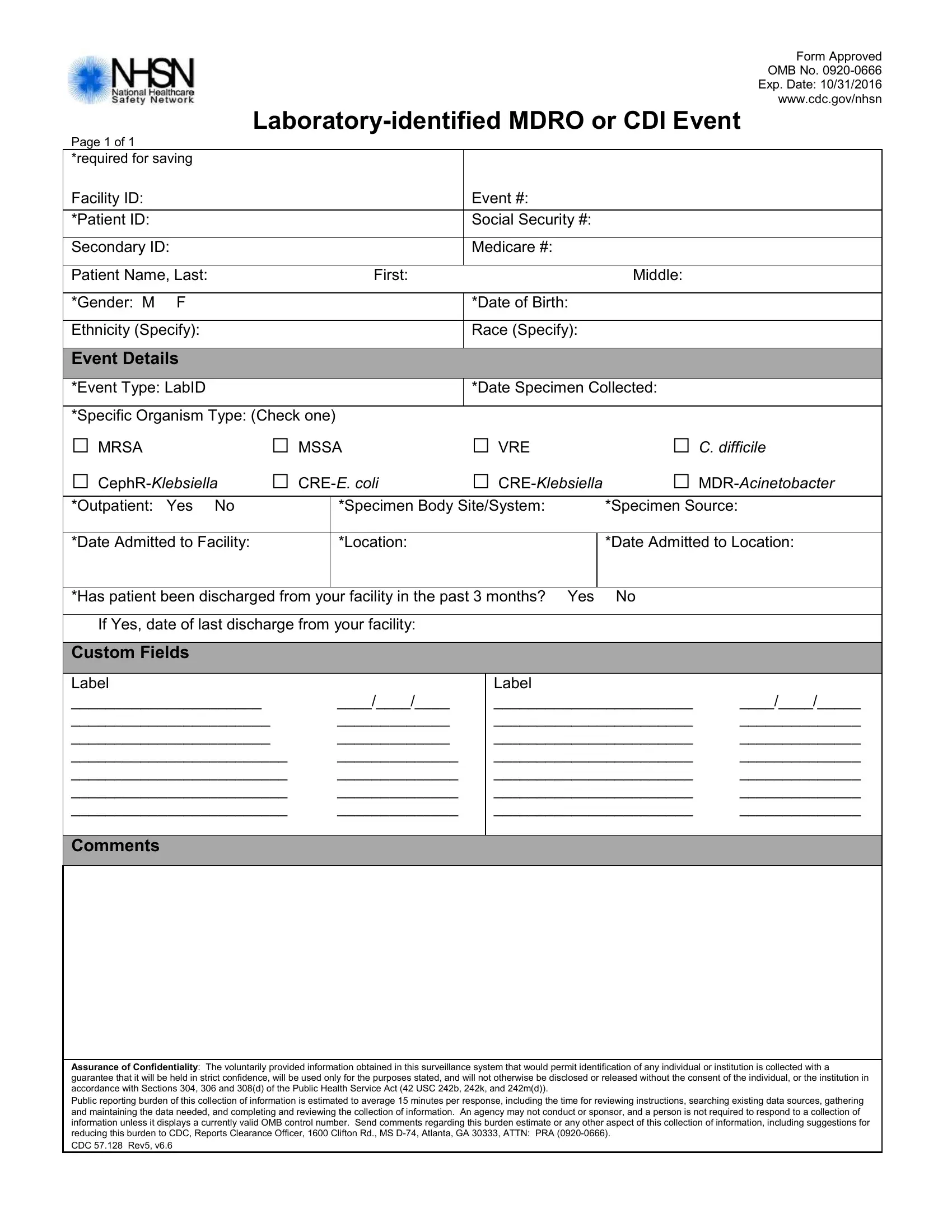
In today's highly digital and interconnected world, precise documentation plays a crucial role in healthcare, particular in monitoring and managing infectious diseases. Among the various tools and forms used, the CDC 57 128 form embodies a vital component in this complex landscape. This specific form, designed for accountability by the Centers for Disease Control and Prevention (CDC), focuses on the surveillance of laboratory-identified Multidrug-resistant organisms (MDRO) and Clostridioides difficile infections (CDI). By requiring detailed patient information, including ID, Social Security number, and demographic details, it ensures a comprehensive approach to tracking infections. Moreover, it highlights key data such as the type of organism detected, specimen details, admission dates, and patient location within the facility, providing a clear snapshot of the event in question. The assurance of confidentiality outlined emphasizes the importance of privacy and trust in public health reporting, underscoring the sensitive nature of the collected data. With a defined public reporting burden, this form not only facilitates the necessary surveillance efforts aimed at controlling and preventing the spread of infections but also reflects the careful balance between data collection and the protection of individual and institutional privacy. As the CDC continues to evolve its strategies and tools in response to emerging healthcare challenges, forms like the CDC 57 128 remain indispensable in the collective effort to safeguard public health.
| Question | Answer |
|---|---|
| Form Name | Form Cdc 57 128 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | 57.128_LabIDEve nt_BLANK laboratory identified mdro or cdi event form |
Form Approved
OMB No.
Exp. Date: 10/31/2016
www.cdc.gov/nhsn
Page 1 of 1
*required for saving
Facility ID: |
|
|
|
|
Event #: |
|
|
||
|
|
|
|
|
|
|
|
|
|
*Patient ID: |
|
|
|
|
Social Security #: |
|
|
||
|
|
|
|
|
|
|
|
|
|
Secondary ID: |
|
|
|
Medicare #: |
|
|
|||
|
|
|
|
|
|
|
|
|
|
Patient Name, Last: |
|
|
First: |
|
|
|
Middle: |
|
|
|
|
|
|
|
|
|
|
|
|
*Gender: M |
F |
|
|
|
*Date of Birth: |
|
|
||
|
|
|
|
|
|
|
|
|
|
Ethnicity (Specify): |
|
|
|
Race (Specify): |
|
|
|||
|
|
|
|
|
|
|
|
|
|
Event Details |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
*Event Type: LabID |
|
|
|
*Date Specimen Collected: |
|
||||
|
|
|
|
|
|
|
|
||
*Specific Organism Type: (Check one) |
|
□ VRE |
□ C. DIFFICILE |
||||||
□ MRSA |
|
□ MSSA |
|||||||
□ |
□ |
□ |
□ |
||||||
*Outpatient: |
Yes No |
|
|
*Specimen Body Site/System: |
*Specimen Source: |
|
|||
|
|
|
|
|
|
|
|
||
*Date Admitted to Facility: |
|
|
*Location: |
|
|
|
*Date Admitted to Location: |
||
|
|
|
|
|
|
||||
*Has patient been discharged from your facility in the past 3 months? Yes |
No |
|
|||||||
|
|
|
|
|
|
||||
If Yes, date of last discharge from your facility: |
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
Custom Fields |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Label |
|
|
|
|
|
Label |
|
|
|
______________________ |
|
|
____/____/____ |
|
_______________________ |
____/____/_____ |
|||
_______________________ |
|
|
_____________ |
|
_______________________ |
______________ |
|||
_______________________ |
|
|
_____________ |
|
_______________________ |
______________ |
|||
_________________________ |
|
______________ |
|
_______________________ |
______________ |
||||
_________________________ |
|
______________ |
|
_______________________ |
______________ |
||||
_________________________ |
|
______________ |
|
_______________________ |
______________ |
||||
_________________________ |
|
______________ |
|
_______________________ |
______________ |
||||
|
|
|
|
|
|
|
|
|
|
Comments
Assurance of Confidentiality: The voluntarily provided information obtained in this surveillance system that would permit identification of any individual or institution is collected with a guarantee that it will be held in strict confidence, will be used only for the purposes stated, and will not otherwise be disclosed or released without the consent of the individual, or the institution in accordance with Sections 304, 306 and 308(d) of the Public Health Service Act (42 USC 242b, 242k, and 242m(d)).
Public reporting burden of this collection of information is estimated to average 15 minutes per response, including the time for reviewing instructions, searching existing data sources, gathering and maintaining the data needed, and completing and reviewing the collection of information. An agency may not conduct or sponsor, and a person is not required to respond to a collection of information unless it displays a currently valid OMB control number. Send comments regarding this burden estimate or any other aspect of this collection of information, including suggestions for reducing this burden to CDC, Reports Clearance Officer, 1600 Clifton Rd., MS
CDC 57.128 Rev5, v6.6