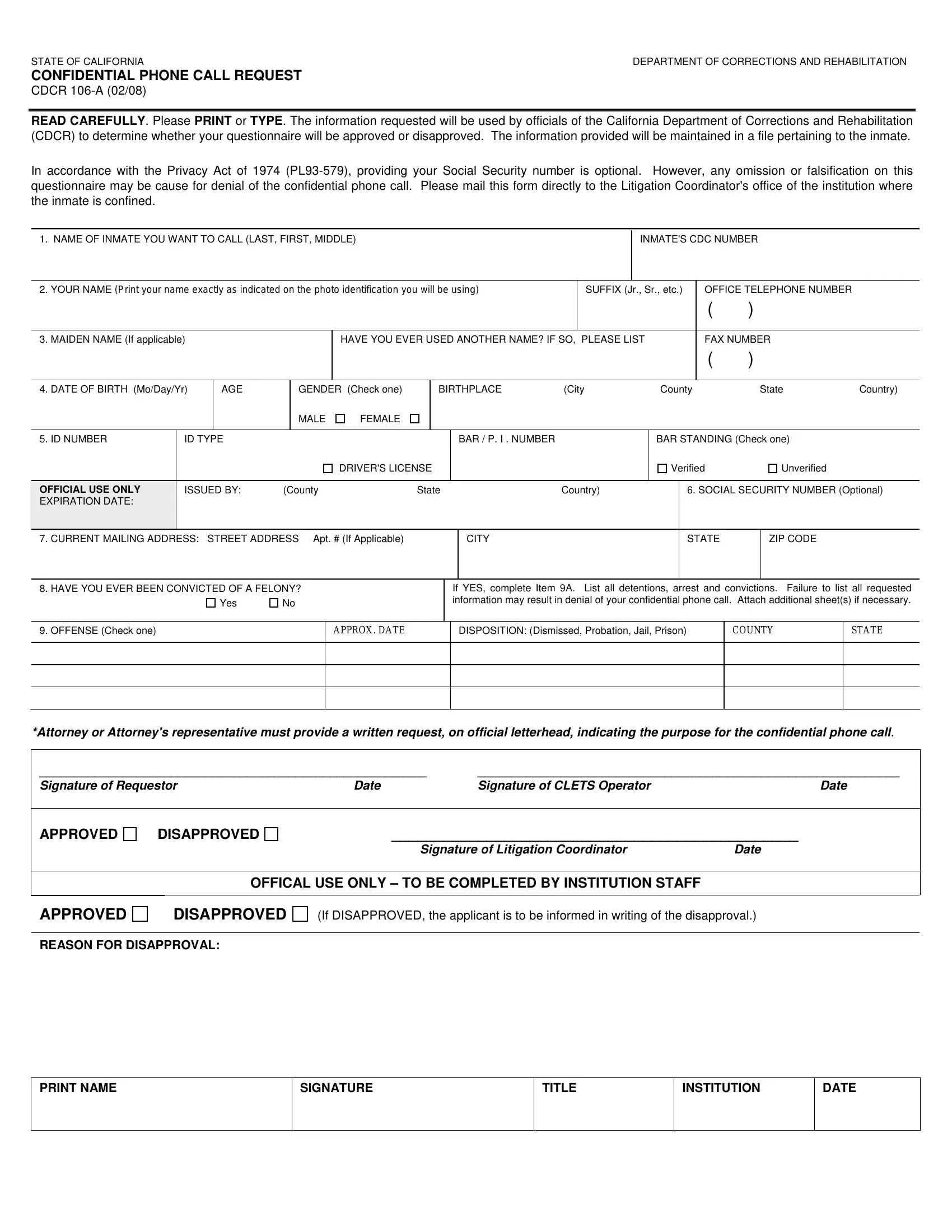
Understanding the intricacies of the CDCR 106-A form is crucial for those seeking a confidential phone call with an inmate housed within the California Department of Corrections and Rehabilitation (CDCDR). This form is a key document used by CDCDR officials to evaluate whether a request for such a confidential communication will be granted. It's important that all information provided on the form is accurate and complete, encompassing everything from personal identification details to any past felony convictions the requester may have. The form also respects the Privacy Act of 1974 regarding the optional provision of Social Security numbers, while emphasizing the importance of honesty in the application process. Failure to accurately disclose information or the falsification of details can lead to the denial of the request. Additionally, the form requires a written statement from an attorney or their representative if the request is being made for legal reasons, ensuring that all communication maintains its intended confidentiality. This comprehensive approach underscores the CDCDR's commitment to maintaining security and privacy, while also accommodating the rights of inmates to communicate with the outside world under certain conditions. By mailing the completed form to the Litigation Coordinator's office at the inmate’s facility, applicants initiate a process that balances legal rights with institutional regulations.
| Question | Answer |
|---|---|
| Form Name | CDCR 106-A Form |
| Form Length | 1 pages |
| Fillable? | Yes |
| Fillable fields | 53 |
| Avg. time to fill out | 10 min 55 sec |
| Other names | SUFFIX, CDC, CLETS, APPROX |
STATE OF CALIFORNIA |
DEPARTMENT OF CORRECTIONS AND REHABILITATION |
CONFIDENTIAL PHONE CALL REQUEST
CDCR
READ CAREFULLY. Please PRINT or TYPE. The information requested will be used by officials of the California Department of Corrections and Rehabilitation (CDCR) to determine whether your questionnaire will be approved or disapproved. The information provided will be maintained in a file pertaining to the inmate.
In accordance with the Privacy Act of 1974
1. NAME OF INMATE YOU WANT TO CALL (LAST, FIRST, MIDDLE) |
|
|
|
|
INMATE'S CDC NUMBER |
|
|||||
|
|
|
|
|
|
|
|
||||
2. YOUR NAME (Print your name exactly as indicated on the photo identification you will be using) |
|
|
SUFFIX (Jr., Sr., etc.) |
OFFICE TELEPHONE NUMBER |
|
||||||
|
|
|
|
|
|
|
|
|
( |
) |
|
|
|
|
|
|
|
|
|||||
3. MAIDEN NAME (If applicable) |
|
|
HAVE YOU EVER USED ANOTHER NAME? IF SO, PLEASE LIST |
FAX NUMBER |
|
||||||
|
|
|
|
|
|
|
|
|
( |
) |
|
|
|
|
|
|
|
|
|
|
|
|
|
4. DATE OF BIRTH (Mo/Day/Yr) |
AGE |
GENDER (Check one) |
BIRTHPLACE |
(City |
|
County |
|
State |
Country) |
||
MALE
FEMALE
5. ID NUMBER |
ID TYPE |
|
|
BAR / P. I . NUMBER |
BAR STANDING (Check one) |
|
|
|
|
DRIVER'S LICENSE |
|
Verified |
Unverified |
|
|
|
|
|
|
|
OFFICIAL USE ONLY |
ISSUED BY: |
(County |
State |
Country) |
6. SOCIAL SECURITY NUMBER (Optional) |
|
EXPIRATION DATE: |
|
|
|
|
|
|
|
|
|
|
|
|
|
7. CURRENT MAILING ADDRESS: STREET ADDRESS Apt. # (If Applicable)
CITY
STATE
ZIP CODE
8. HAVE YOU EVER BEEN CONVICTED OF A FELONY?
Yes |
No |
If YES, complete Item 9A. List all detentions, arrest and convictions. Failure to list all requested information may result in denial of your confidential phone call. Attach additional sheet(s) if necessary.
9. OFFENSE (Check one)
APPROX. DATE
DISPOSITION: (Dismissed, Probation, Jail, Prison)
COUNTY
STATE
*Attorney or Attorney's representative must provide a written request, on official letterhead, indicating the purpose for the confidential phone call.
________________________________________________________ |
_____________________________________________________________ |
||
Signature of Requestor |
Date |
Signature of CLETS Operator |
Date |
APPROVED
DISAPPROVED
_______________________________________________
Signature of Litigation Coordinator |
Date |
OFFICAL USE ONLY – TO BE COMPLETED BY INSTITUTION STAFF
APPROVED
DISAPPROVED
(If DISAPPROVED, the applicant is to be informed in writing of the disapproval.)
REASON FOR DISAPPROVAL:
PRINT NAME
SIGNATURE
TITLE
INSTITUTION
DATE