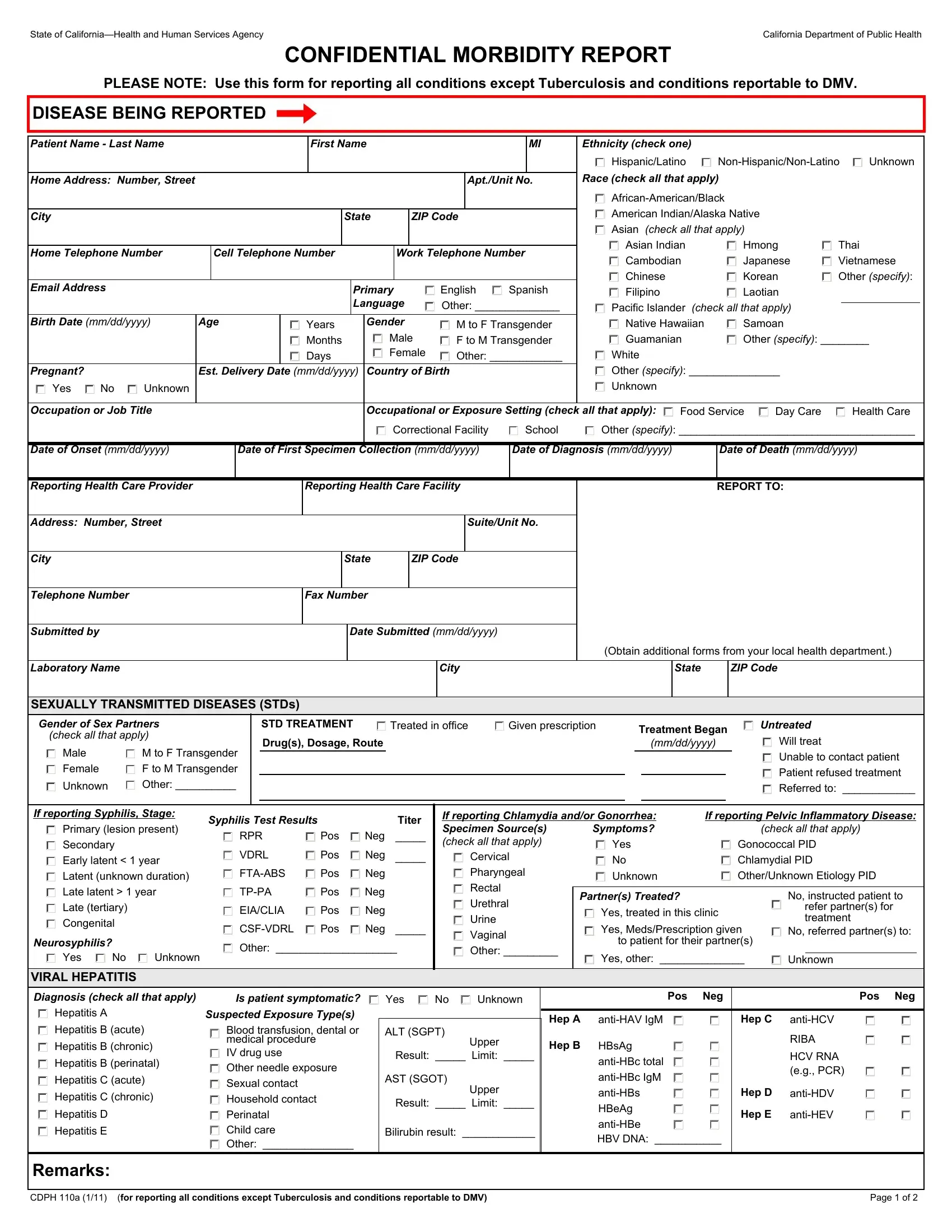
In the complex landscape of public health reporting and management, the CDPH 110A form emerges as a critical document within California's healthcare infrastructure. Designed and mandated by the State of California—Health and Human Services Agency, and specifically utilized by the California Department of Public Health, this form assumes a vital role in the confidential morbidity reporting process. It stipulates a structured approach for healthcare professionals to report a wide spectrum of conditions, excluding Tuberculosis and conditions reportable to the Department of Motor Vehicles (DMV). The comprehensive nature of the form captures detailed patient information including but not limited to ethnicity, race, gender, birth details, contact information, and linguistic preference. Significantly, the form delves into specifics regarding the disease being reported, exposure settings, onset and diagnosis dates, and detailed treatment information for sexually transmitted diseases (STDs), as well as viral hepatitis—highlighting its pivotal role in disease surveillance and public health initiative. Equally important is the section dedicated to the reporting healthcare provider and facility, ensuring a clear channel for communication and follow-up. This intricate form not only facilitates a systematic reporting to health authorities but also underscores the importance of accurate data collection in implementing effective public health strategies and interventions.
| Question | Answer |
|---|---|
| Form Name | Form Cdph 110A |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | CMRcdph0110a confidential morbidity report san bernardino county form |
State of |
California Department of Public Health |
CONFIDENTIAL MORBIDITY REPORT
PLEASE NOTE: Use this form for reporting all conditions except Tuberculosis and conditions reportable to DMV.
DISEASE BEING REPORTED
Patient Name - Last Name |
|
|
|
|
|
|
|
First Name |
|
|
|
|
|
|
|
|
|
|
MI |
Ethnicity (check one) |
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Hispanic/Latino |
Unknown |
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Race (check all that apply) |
|
|
|
|
|
|
|||||
Home Address: Number, Street |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Apt./Unit No. |
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
American Indian/Alaska Native |
|
|
|
|
|
|
|||
City |
|
|
|
|
|
|
|
|
|
|
State |
|
|
|
ZIP Code |
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Asian (check all that apply) |
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Asian Indian |
Hmong |
Thai |
|
|
|
||||
Home Telephone Number |
|
Cell Telephone Number |
|
|
|
Work Telephone Number |
|
|
Cambodian |
Japanese |
Vietnamese |
|||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Chinese |
|
Korean |
Other (specify): |
||||||
Email Address |
|
|
|
|
|
|
|
|
|
|
|
|
English |
Spanish |
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
Primary |
|
|
|
|
Filipino |
|
Laotian |
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Language |
Other: ______________ |
|
|
Pacific Islander (check all that apply) |
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
Birth Date (mm/dd/yyyy) |
Age |
|
|
|
|
Years |
Gender |
|
M to F Transgender |
|
|
Native Hawaiian |
Samoan |
|
|
|
|
|
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
Months |
|
|
Male |
|
F to M Transgender |
|
|
Guamanian |
Other (specify): ________ |
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
Days |
|
|
Female |
|
Other: ____________ |
|
|
White |
|
|
|
|
|
|
|
|
||||||||||||
Pregnant? |
|
|
Est. Delivery Date (mm/dd/yyyy) |
Country of Birth |
|
|
|
|
Other (specify): _______________ |
|
|
|
|
|
||||||||||||||||||||||||||
|
|
|
Yes |
No |
Unknown |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Unknown |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Occupation or Job Title |
|
|
|
|
|
|
|
|
|
|
|
Occupational or Exposure Setting (check all that apply): |
|
Food Service |
Day Care |
|
Health Care |
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Correctional Facility |
School |
|
Other (specify): _______________________________________ |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||
Date of Onset (mm/dd/yyyy) |
|
|
Date of First Specimen Collection (mm/dd/yyyy) |
Date of Diagnosis (mm/dd/yyyy) |
|
Date of Death (mm/dd/yyyy) |
|
|
|
|||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
Reporting Health Care Provider |
|
|
|
|
|
|
Reporting Health Care Facility |
|
|
|
|
|
|
|
REPORT TO: |
|
|
|
|
|
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
Address: Number, Street |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Suite/Unit No. |
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
City |
|
|
|
|
|
|
|
|
|
|
State |
|
|
|
ZIP Code |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Telephone Number |
|
|
|
|
|
|
|
Fax Number |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
Submitted by |
|
|
|
|
|
|
|
|
|
|
|
Date Submitted (mm/dd/yyyy) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(Obtain additional forms from your local health department.) |
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Laboratory Name
City
State |
ZIP Code |
SEXUALLY TRANSMITTED DISEASES (STDs)
Gender of Sex Partners
(check all that apply)
Male |
M to F Transgender |
Female |
F to M Transgender |
Unknown |
Other: __________ |
STD TREATMENT |
|
Treated in office |
Given prescription |
Treatment Began |
|
|
Untreated |
Drug(s), Dosage, Route |
|
|
|
|
Will treat |
||
|
|
(mm/dd/yyyy) |
|
|
|||
|
|
|
|
|
|
|
Unable to contact patient |
Patient refused treatment
Referred to: ____________
If reporting Syphilis, Stage:
Primary (lesion present) Secondary
Early latent < 1 year Latent (unknown duration)
Late latent > 1 year
Late (tertiary)
Congenital
Neurosyphilis?
Yes No Unknown
Syphilis Test Results |
|
|
Titer |
||
RPR |
|
|
Pos |
Neg |
_____ |
|
|||||
VDRL |
Pos |
Neg |
_____ |
||
Pos |
Neg |
|
|||
Pos |
Neg |
|
|||
EIA/CLIA |
Pos |
Neg |
|
||
Pos |
Neg |
_____ |
|||
Other: ____________________
If reporting Chlamydia and/or Gonorrhea: |
If reporting Pelvic Inflammatory Disease: |
||||||||||||
Specimen Source(s) |
|
Symptoms? |
|
|
|
(check all that apply) |
|||||||
(check all that apply) |
|
|
|
|
Yes |
|
|
Gonococcal PID |
|||||
|
|
||||||||||||
|
|
Cervical |
|
|
|
|
No |
|
|
Chlamydial PID |
|||
|
|
|
|
|
|
|
|
||||||
|
|
Pharyngeal |
|
|
|
|
|
|
|||||
|
|
|
|
|
|
Unknown |
|
|
Other/Unknown Etiology PID |
||||
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|||||
|
|
Rectal |
|
|
|
|
|
|
|
|
|
|
|
|
|
Partner(s) Treated? |
|
|
|
No, instructed patient to |
|||||||
|
|
Urethral |
|
|
|
||||||||
|
|
|
|
|
Yes, treated in this clinic |
refer partner(s) for |
|||||||
|
|
|
|
|
|
||||||||
|
|
Urine |
|
|
|
treatment |
|||||||
|
|
|
|
|
Yes, Meds/Prescription given |
||||||||
|
|
Vaginal |
|
|
|
No, referred partner(s) to: |
|||||||
|
|
|
|
|
|
to patient for their partner(s) |
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
||||
|
|
Other: _________ |
|
|
|
Yes, other: ______________ |
|
|
|
||||
|
|
|
|
|
Unknown |
||||||||
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
VIRAL HEPATITIS
Diagnosis (check all that apply)
Hepatitis A
Hepatitis B (acute)
Hepatitis B (chronic)
Hepatitis B (perinatal)
Hepatitis C (acute)
Hepatitis C (chronic)
Hepatitis D
Hepatitis E
|
|
Is patient symptomatic? |
Yes |
No |
Unknown |
Suspected Exposure Type(s) |
|
|
|
||
|
|
Blood transfusion, dental or |
ALT (SGPT) |
|
|
|
|
|
|||
|
|
medical procedure |
|
|
Upper |
|
|
|
|
||
|
|
|
|
|
|
|
|
IV drug use |
Result: _____ |
Limit: _____ |
|
|
|
Other needle exposure |
|
|
|
|
|
Sexual contact |
AST (SGOT) |
|
|
|
|
|
|
Upper |
|
|
|
Household contact |
|
|
|
|
|
Result: _____ |
Limit: _____ |
||
|
|
|
|||
|
|
Perinatal |
|
|
|
|
|
Child care |
Bilirubin result: ____________ |
||
|
|
|
|||
|
|
Other: _______________ |
|
|
|
|
|
|
|
|
|
|
Pos |
Neg |
|
Pos Neg |
||||
|
|
|
|
|
|
|
||
Hep A |
|
Hep C |
||||||
Hep B |
HBsAg |
|
|
|
|
RIBA |
|
|
|
|
|
|
|
||||
|
|
|
|
|||||
|
|
|
|
HCV RNA |
||||
|
|
|
||||||
|
|
|
(e.g., PCR) |
|||||
|
|
|
||||||
|
|
|
|
|
|
|||
|
|
Hep D |
||||||
|
HBeAg |
|
Hep E |
|||||
|
|
|||||||
|
|
|
|
|
|
|||
|
HBV DNA: ___________ |
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
Remarks:
CDPH 110a (1/11) (for reporting all conditions except Tuberculosis and conditions reportable to DMV) |
Page 1 of 2 |
State of |
California Department of Public Health |
CDPH 110a (1/11) |
Page 2 of 2 |