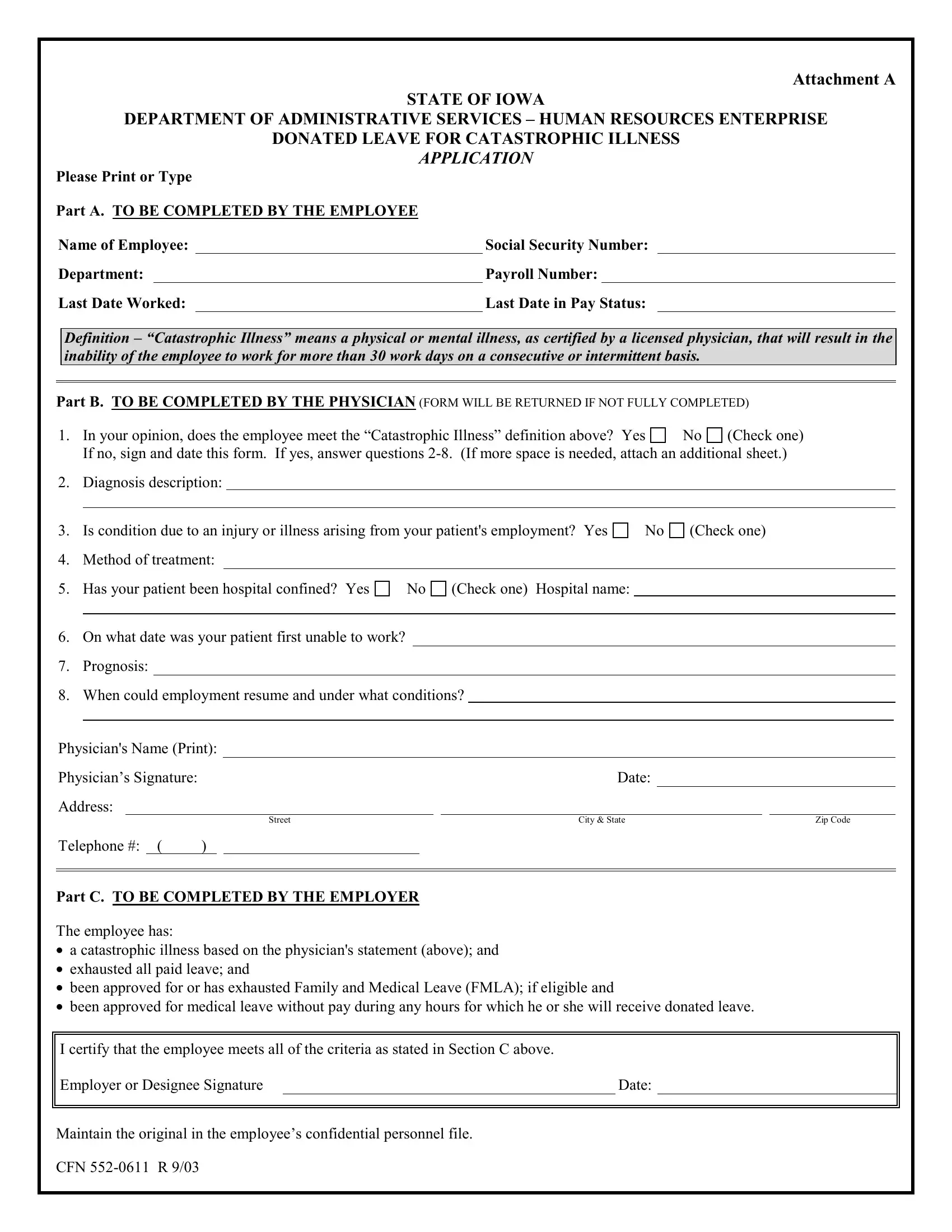
The CFN 552-0611 form is a crucial document for employees within the State of Iowa, particularly those facing severe health challenges. Managed by the Department of Administrative Services – Human Resources Enterprise, this form facilitates the process for applying for donated leave in the event of a catastrophic illness. By definition within this context, a catastrophic illness refers to any physical or mental condition, certified by a licensed physician, that significantly disrupts an employee's ability to work for an extended period. The form itself is meticulously divided into sections that require detailed input from both the employee suffering from the illness and their physician. It starts with personal details and work-related information provided by the employee, followed by a comprehensive assessment from a healthcare professional regarding the illness, its causes, prognosis, and recommended treatment plan. Furthermore, the document outlines specific criteria regarding the employee's eligibility for donated leave, including the exhaustion of all paid leave and whether they have been approved for or exhausted Family and Medical Leave Act (FMLA) entitlements. The final section necessitates confirmation from the employer or designated representative, ensuring all stated conditions are met. This form underscores a compassionate approach to employee welfare, enabling a support system through donated leave for those enduring significant health issues.
| Question | Answer |
|---|---|
| Form Name | Form Cfn 552 0611 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | 552 0611_catastroph ic_leave_reques t internal revenue service catastrophic illness definition form |
Attachment A
STATE OF IOWA
DEPARTMENT OF ADMINISTRATIVE SERVICES – HUMAN RESOURCES ENTERPRISE
DONATED LEAVE FOR CATASTROPHIC ILLNESS
APPLICATION
Please Print or Type
Part A. TO BE COMPLETED BY THE EMPLOYEE |
|
|
|
||
Name of Employee: |
|
Social Security Number: |
|
||
Department: |
|
Payroll Number: |
|
||
Last Date Worked: |
|
Last Date in Pay Status: |
|
||
Definition – “Catastrophic Illness” means a physical or mental illness, as certified by a licensed physician, that will result in the inability of the employee to work for more than 30 work days on a consecutive or intermittent basis.
Part B. TO BE COMPLETED BY THE PHYSICIAN (FORM WILL BE RETURNED IF NOT FULLY COMPLETED)
1. |
In your opinion, does the employee meet the “Catastrophic Illness” definition above? Yes |
No |
(Check one) |
||
|
If no, sign and date this form. If yes, answer questions |
||||
2. |
Diagnosis description: |
|
|
||
|
|
|
|
|
|
3. Is condition due to an injury or illness arising from your patient's employment? Yes
No
(Check one)
4. Method of treatment:
5. Has your patient been hospital confined? Yes |
No |
(Check one) Hospital name: |
6.On what date was your patient first unable to work?
7.Prognosis:
8.When could employment resume and under what conditions?
Physician's Name (Print): |
|
|
|
|
|
||||||
Physician’s Signature: |
|
|
|
|
|
Date: |
|
|
|
||
Address: |
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
Street |
|
City & State |
|
|
Zip Code |
|
Telephone #: ( |
) |
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Part C. TO BE COMPLETED BY THE EMPLOYER
The employee has:
•a catastrophic illness based on the physician's statement (above); and
•exhausted all paid leave; and
•been approved for or has exhausted Family and Medical Leave (FMLA); if eligible and
•been approved for medical leave without pay during any hours for which he or she will receive donated leave.
I certify that the employee meets all of the criteria as stated in Section C above.
Employer or Designee Signature |
|
Date: |
Maintain the original in the employee’s confidential personnel file.
CFN