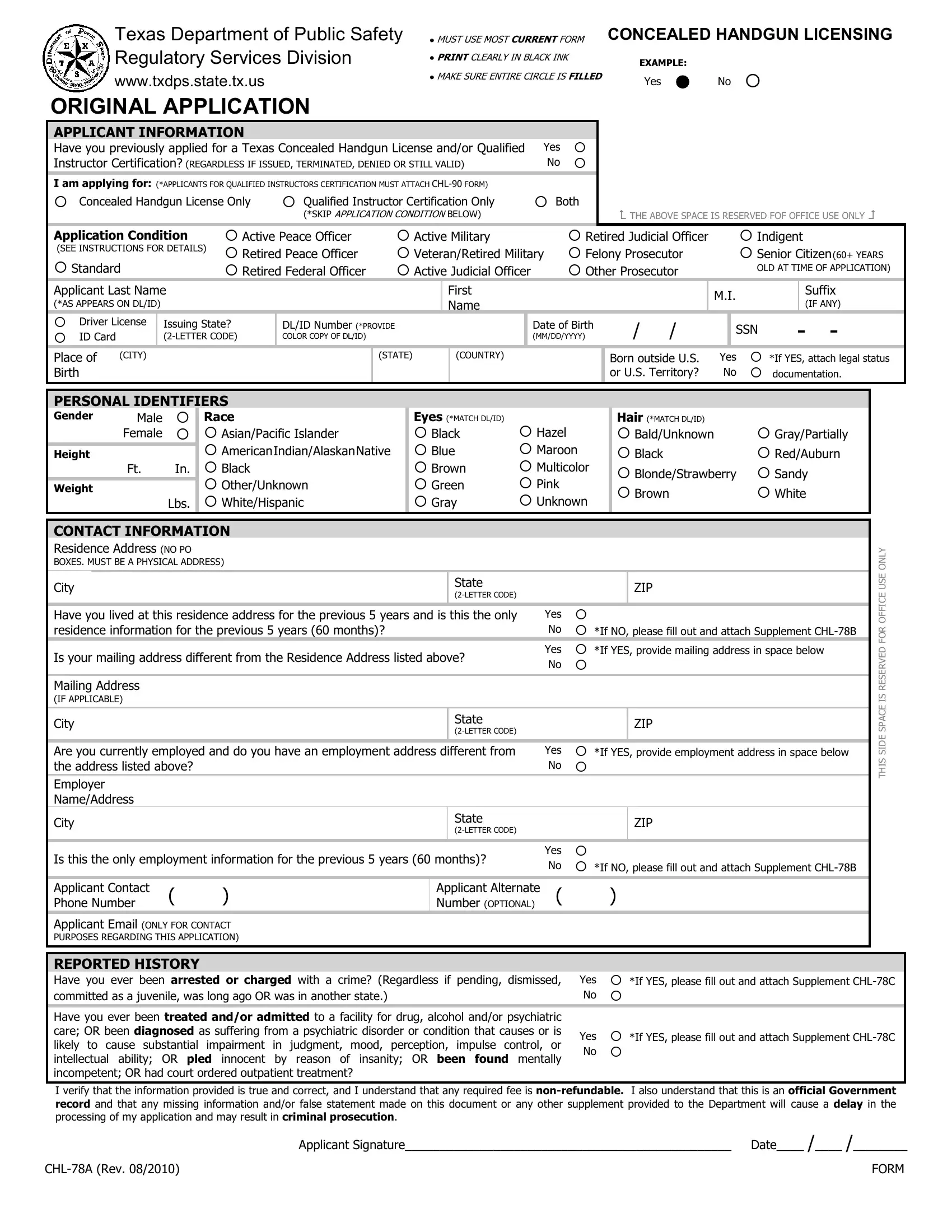
The journey to legally carry a concealed handgun in Texas navigates through a thorough documentation process orchestrated by the Texas Department of Public Safety, converging at the crucial dock of the CHL 78A form. This document serves as the original application required for individuals seeking a Concealed Handgun License (CHL) or opting for Qualified Instructor Certification within the state's jurisdiction. Precision in completion, highlighted by the mandate to use only black ink, underscores its importance in the regulatory framework overseen by the Concealed Handgun Licensing unit of the Regulatory Services Division. The form not only caters to first-time applicants but also extends its realm to encompass those with previous applications, regardless of the outcome (issued, terminated, denied, or still valid), thereby weaving a web of inclusivity around varied applicant profiles. Integral to the process is the provision for applicants to declare their specific application condition, spanning categories from active military personnel to senior citizens, each carrying its own set of instructions and implications. Personal identifiers, a comprehensive contact information section, employment details, and a candid disclosure of any criminal or psychiatric history further sculpt the application, ensuring a multifaceted view of the applicant's background. The CHL 78A form, meticulously structured and demanding attention to detail, stands as a testimonial to Texas’s commitment to safety and regulation in the area of concealed firearms.
| Question | Answer |
|---|---|
| Form Name | Form Chl 78A |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | CHL 78A how to fill out chl 78a rev 082010 form |
Texas Department of Public Safety |
MUST USE MOST CURRENT FORM CONCEALED HANDGUN LICENSING |
||
Regulatory Services Division |
PRINT CLEARLY IN BLACK INK |
EXAMPLE: |
|
www.txdps.state.tx.us |
MAKE SURE ENTIRE CIRCLE IS FILLED |
Yes |
No |
|
|||
ORIGINAL APPLICATION
APPLICANT INFORMATION
Have you previously applied for a Texas Concealed Handgun License and/or Qualified |
Yes |
|
Instructor Certification? (REGARDLESS IF ISSUED, TERMINATED, DENIED OR STILL VALID) |
No |
|
Iam applying for: (*APPLICANTS FOR QUALIFIED INSTRUCTORS CERTIFICATION MUST ATTACH
Concealed Handgun License Only |
Qualified Instructor Certification Only |
Both |
|
(*SKIP APPLICATION CONDITION BELOW) |
|
THE ABOVE SPACE IS RESERVED FOF OFFICE USE ONLY
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Application Condition |
Active Peace Officer |
Active Military |
Retired Judicial Officer |
|
|
|
Indigent |
|||||||
(SEE INSTRUCTIONS FOR DETAILS) |
Retired Peace Officer |
Veteran/Retired Military |
Felony Prosecutor |
|
|
|
Senior Citizen(60+ YEARS |
|||||||
Standard |
Retired Federal Officer |
Active Judicial Officer |
Other Prosecutor |
|
|
|
OLD AT TIME OF APPLICATION) |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Applicant Last Name |
|
|
First |
|
|
|
M.I. |
|
Suffix |
|||||
(*AS APPEARS ON DL/ID) |
|
|
Name |
|
|
|
|
|
|
(IF ANY) |
||||
|
|
|
|
|
|
|
|
|
||||||
|
Driver License |
Issuing State? |
DL/ID Number (*PROVIDE |
|
Date of Birth |
||
|
ID Card |
|
COLOR COPY OF DL/ID) |
|
(MM/DD/YYYY) |
||
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
Place of |
(CITY) |
|
|
(STATE) |
(COUNTRY) |
||
Birth |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
/ |
/ |
|
SSN |
- |
- |
|
Born outside U.S. |
Yes |
*If YES, attach legal status |
||||
or U.S. Territory? |
No |
documentation. |
||||
PERSONAL IDENTIFIERS
|
Gender |
Male |
|
Race |
Eyes (*MATCH DL/ID) |
Hair (*MATCH DL/ID) |
|
|
|
|
Female |
|
Asian/Pacific Islander |
Black |
Hazel |
Bald/Unknown |
Gray/Partially |
|
Height |
|
|
AmericanIndian/AlaskanNative |
Blue |
Maroon |
Black |
Red/Auburn |
|
|
|
||||||
|
|
Ft. |
In. |
Black |
Brown |
Multicolor |
Blonde/Strawberry |
Sandy |
|
Weight |
|
|
Other/Unknown |
Green |
Pink |
Brown |
White |
|
|
|
Lbs. |
White/Hispanic |
Gray |
Unknown |
||
|
|
|
|
|
|
|
|
|
CONTACT INFORMATION
Residence Address (NO PO
BOXES. MUST BE A PHYSICAL ADDRESS)
City |
|
|
|
|
State |
|
|
ZIP |
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|||
Have you lived at this residence address for the previous 5 years and is this the only |
Yes |
|
|||||||
residence information for the previous 5 years (60 months)? |
|
|
No |
*If NO, please fill out and attach Supplement |
|||||
Is your mailing address different from the Residence Address listed above? |
Yes |
*If YES, provide mailing address in space below |
|||||||
No |
|
||||||||
|
|
|
|
|
|
||||
Mailing Address |
|
|
|
|
|
|
|
||
(IF APPLICABLE) |
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
City |
|
|
|
State |
|
|
ZIP |
||
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|||
Are you currently employed and do you have an employment address different from |
Yes |
*If YES, provide employment address in space below |
|||||||
the address listed above? |
|
|
|
No |
|
||||
Employer |
|
|
|
|
|
|
|
||
Name/Address |
|
|
|
|
|
|
|
||
City |
|
|
|
State |
|
|
ZIP |
||
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
||
Is this the only employment information for the previous 5 years (60 months)? |
Yes |
|
|||||||
No |
*If NO, please fill out and attach Supplement |
||||||||
|
|
|
|
|
|
||||
Applicant Contact |
( |
) |
Applicant Alternate |
( |
) |
|
|||
Phone Number |
Number (OPTIONAL) |
|
|||||||
Applicant Email (ONLY FOR CONTACT
PURPOSES REGARDING THIS APPLICATION)
THIS SIDE SPACE IS RESERVED FOR OFFICE USE ONLY
REPORTED HISTORY
Have you ever been arrested or charged with a crime? (Regardless if pending, dismissed, |
Yes |
*If YES, please fill out and attach Supplement |
|
committed as a juvenile, was long ago OR was in another state.) |
No |
|
|
Have you ever been treated and/or admitted to a facility for drug, alcohol and/or psychiatric |
|
|
|
care; OR been diagnosed as suffering from a psychiatric disorder or condition that causes or is |
Yes |
*If YES, please fill out and attach Supplement |
|
likely to cause substantial impairment in judgment, mood, perception, impulse control, or |
No |
|
|
intellectual ability; OR pled innocent by reason of insanity; OR been found mentally |
|||
|
|
||
incompetent; OR had court ordered outpatient treatment? |
|
|
I verify that the information provided is true and correct, and I understand that any required fee is
Applicant Signature________________________________________________ |
Date____ /____ /________ |
FORM |