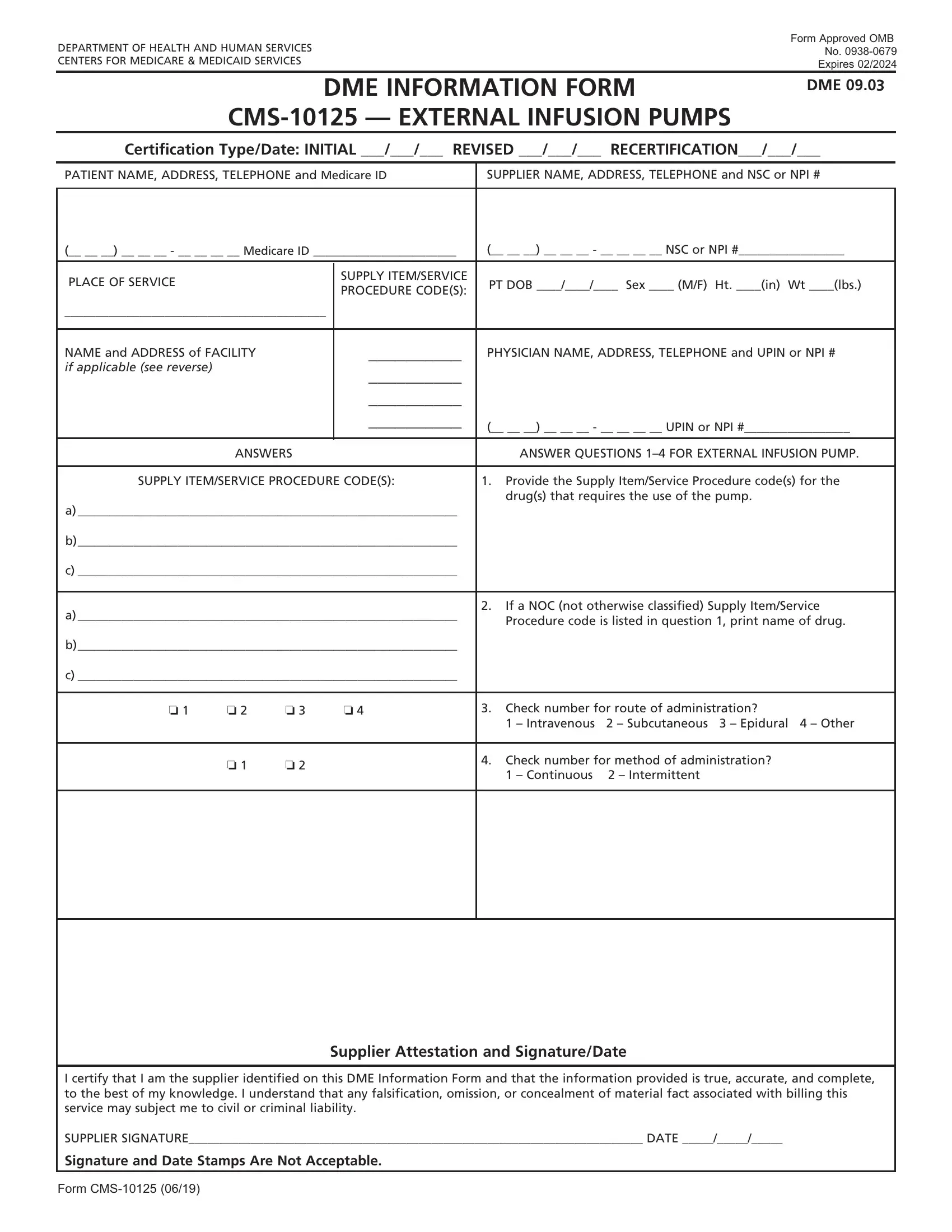
The CMS-10125 form, fundamentally designed by the Department of Health and Human Services and approved by the Office of Management and Budget (OMB No. 0938-0679), serves the crucial purpose of facilitating the provision of External Infusion Pumps under the Centers for Medicare & Medicaid Services. With an expiration date set for February 2024, this Durable Medical Equipment (DME) Information Form is integral for certifying initial, revised, or recertified claims for service. The form encapsulates various segments requiring detailed patient information, supplier data, and specific guidelines to accurately code the supply item/service procedure. Furthermore, it delineates a section dedicated to the physician's details, including their name, address, telephone number, and UPIN or NPI number if applicable. Questions aimed at unearthing clinical specifics about the item or service billed are a part of this comprehensive form, which also insists on a supplier attestation to validate the authenticity and accuracy of the information provided. Ultimately, the CMS-10125 form is pivotal in ensuring that the administration and billing of external infusion pumps are handled in a structured and standardized manner, safeguarding the alignment with regulatory compliance and aiding in the streamlined processing of Medicare claims.
| Question | Answer |
|---|---|
| Form Name | Form Cms 10125 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | dif form sample, form recertification cms, cms dme forms print, form recertification cms online |
