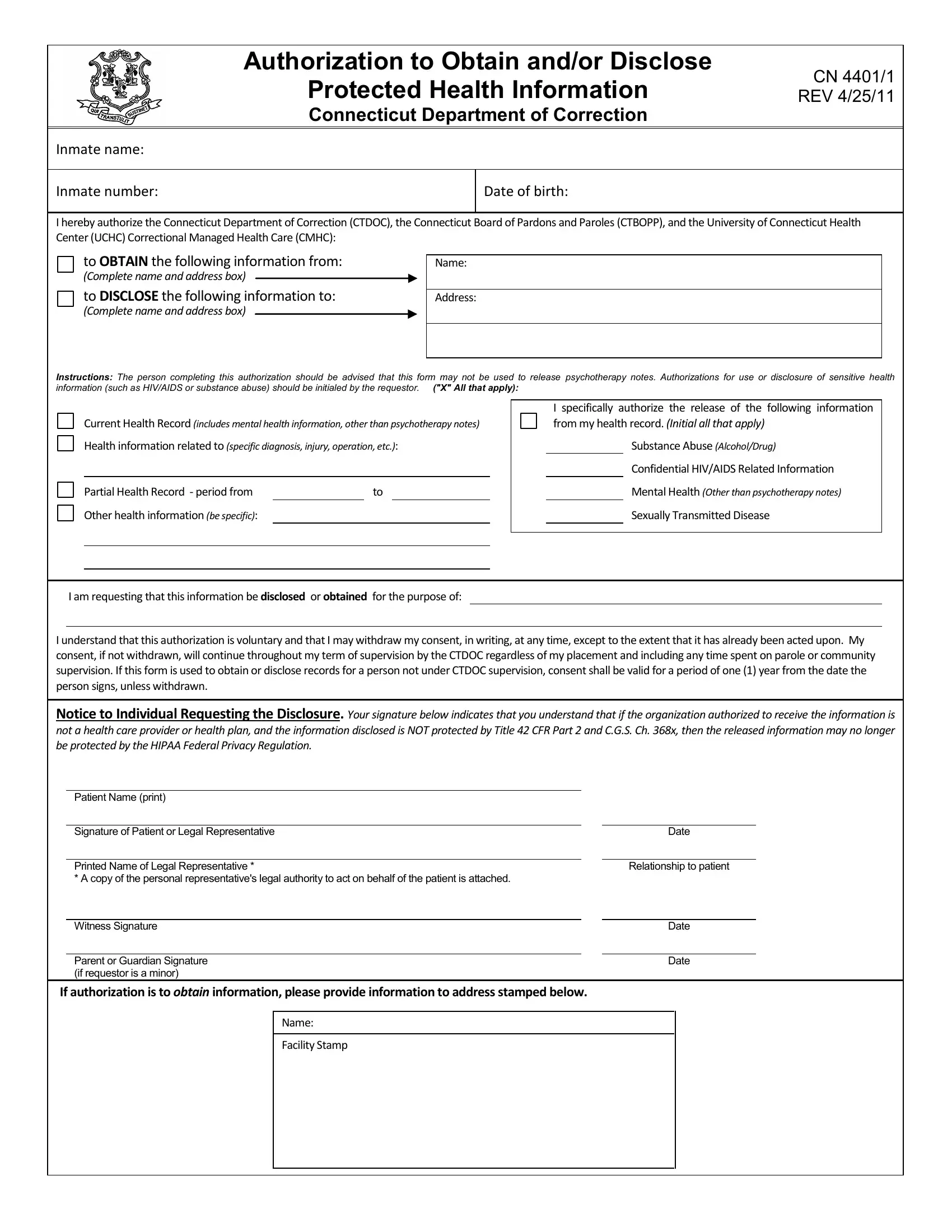
The CN 4401 form, officially titled "Authorization to Obtain and/or Disclose Protected Health Information," serves as a crucial document within the Connecticut Department of Correction. This comprehensive form is designed to authorize the acquisition and release of protected health information for inmates within the jurisdiction of the Connecticut Department of Correction (CTDOC), the Connecticut Board of Pardons and Paroles (CTBOPP), and the University of Connecticut Health Center (UCHC) Correctional Managed Health Care (CMHC). The form meticulously outlines the process for consenting to both obtain and disclose various types of health information, including but not limited to substance abuse records, HIV/AIDS related information, mental health details (excluding psychotherapy notes), and information related to sexually transmitted diseases. Intended users are cautioned about the form's incapability to release psychotherapy notes and the necessity of specifying authorizations for sensitive health information disclosures. Furthermore, the form makes clear that the consent provided is voluntary and can be withdrawn in writing at any point, with specific durations for consent outlined depending on the individual's status with CTDOC. It additionally highlights the legal implications for recipients of such information, emphasizing restrictions on further disclosure set by federal and state laws, particularly concerning information related to HIV, behavioral health, alcohol, or drug abuse. This attention to legal and ethical guidelines underscores the form's purpose in safeguarding inmate privacy while enabling necessary healthcare communications.
| Question | Answer |
|---|---|
| Form Name | Form Cn 4401 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | UCHC, CFR, CN, Authorizations |
Authorization to Obtain and/or Disclose
Protected Health Information |
CN 4401/1 |
REV 4/25/11 |
|
Connecticut Department of Correction |
|
Inmate name:
Inmate number:
Date of birth:
I hereby authorize the Connecticut Department of Correction (CTDOC), the Connecticut Board of Pardons and Paroles (CTBOPP), and the University of Connecticut Health Center (UCHC) Correctional Managed Health Care (CMHC):
to OBTAIN the following information from:
(Complete name and address box)
to DISCLOSE the following information to:
(Complete name and address box)
Name:
Address:
Instructions: The person completing this authorization should be advised that this form may not be used to release psychotherapy notes. Authorizations for use or disclosure of sensitive health information (such as HIV/AIDS or substance abuse) should be initialed by the requestor. ("X" All that apply):
Current Health Record (includes mental health information, other than psychotherapy notes)
Health information related to (specific diagnosis, injury, operation, etc.):
Partial Health Record - period from |
|
to |
Other health information (be specific):
I specifically authorize the release of the following information from my health record. (Initial all that apply)
Substance Abuse (Alcohol/Drug)
Confidential HIV/AIDS Related Information
Mental Health (Other than psychotherapy notes)
Sexually Transmitted Disease
I am requesting that this information be disclosed or obtained for the purpose of:
I understand that this authorization is voluntary and that I may withdraw my consent, in writing, at any time, except to the extent that it has already been acted upon. My consent, if not withdrawn, will continue throughout my term of supervision by the CTDOC regardless of my placement and including any time spent on parole or community supervision. If this form is used to obtain or disclose records for a person not under CTDOC supervision, consent shall be valid for a period of one (1) year from the date the person signs, unless withdrawn.
Notice to Individual Requesting the Disclosure. Your signature below indicates that you understand that if the organization authorized to receive the information is not a health care provider or health plan, and the information disclosed is NOT protected by Title 42 CFR Part 2 and C.G.S. Ch. 368x, then the released information may no longer be protected by the HIPAA Federal Privacy Regulation.
Patient Name (print)
Signature of Patient or Legal Representative
Printed Name of Legal Representative *
* A copy of the personal representative's legal authority to act on behalf of the patient is attached.
Witness Signature
Parent or Guardian Signature (if requestor is a minor)
Date
Relationship to patient
Date
Date
If authorization is to obtain information, please provide information to address stamped below.
Name:
Facility Stamp
Authorization to Obtain and/or Disclose
Protected Health Information |
CN 4401/2 |
REV 4/25/11 |
|
Connecticut Department of Correction |
|
Inmate name:
Inmate number:
Date of birth:
Notice to Recipients:
As the recipient of this information, you may use this information only for the stated purpose. You may disclose this information to another party ONLY:
With written authorization from the patient of his or her legal representative;
As required or authorized by state and/or federal law; or,
If urgently needed for the patient's continued care.
If this disclosure contains information relating to HIV, behavioral health, alcohol or drug abuse education, training, treatment, rehabilitation, or research, the following shall apply: This information has been disclosed to you from records whose confidentiality is protected by federal law. Federal regulations (Title 42 CFR Part 2 and C.G.S. Ch. 368x) prohibit you from making any further disclosure of it without the specific written consent of the person to whom it pertains, or as otherwise permitted by such regulations. A general authorization for the release of medical or other information is NOT sufficient for this purpose. State law contains similar provisions with respect to confidential HIV information, C.G.S.
Notice to Individual Requesting the Disclosure:
I understand that I may inspect and copy the information to be used and disclosed under this authorization and that I may receive a copy of this signed authorization form. There may be a fee associated with the copying, not to exceed what Connecticut State law authorizes.
CTDOC, CTBOPP, UCHC/CMHC, and their employees, officers, and physicians are hereby released from any legal responsibility or liability for disclosure of the above information to the extent indicated and authorized herein.
I understand that CTDOC, CTBOPP or UCHC/CMHC may not condition present or future treatment on the provision of this authorization.
REQUEST TO WITHDRAW AUTHORIZATION (except to the extent that the release has already been acted on)
I withdraw my consent to disclose or obtain health information authorized above.
Patient Name (print) |
|
|
|
|
|
Signature of Patient or Legal Representative |
|
Date |
|
|
|
Witness Signature |
|
Date |
|
|
|
Parent or Guardian Signature |
|
Date |
(if requestor is a minor) |
|
|