Form CR 3 is a form used to request a correction to your individual income tax return. If you find an error on your return, use this form to request the IRS correct it. The form must be submitted within 3 years of the original filing date or 2 years after the date of the payment of the tax, whichever is later. It's important to note that you can only file Form CR 3 for errors related to your own return - not those of another taxpayer. So if you notice an error on your return, be sure to submit Form CR 3 as soon as possible!
| Question | Answer |
|---|---|
| Form Name | Form Cr 3 |
| Form Length | 4 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min |
| Other names | txdot cr 3 form, cr 3 form, texas cr 3 form 2019, texas peace officer's crash report code sheet 2021 |

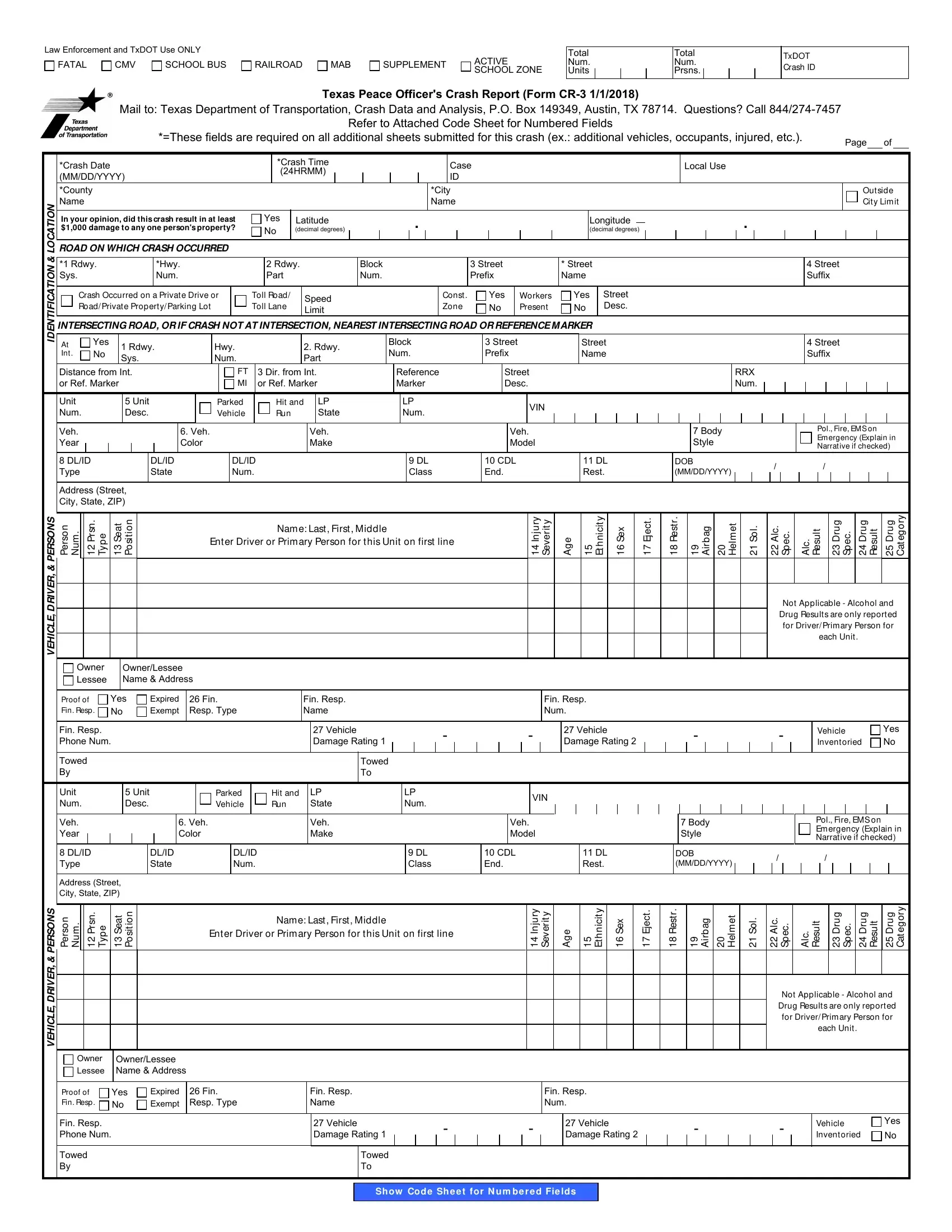
Law Enforcement and TxDOT Use ONLY |
|
||
FATAL |
CMV |
SCHOOL BUS |
RAILROAD |
MAB
SUPPLEMENT
ACTIVE |
Total |
Num. |
|
SCHOOL ZONE |
Units |
|
|
Total
Num.
Prsns.
TxDOT Crash ID
Texas Peace Officer's Crash Report (Form |
|
Mail to: Texas Department of Transportation, Crash Data and Analysis, P.O. Box 149349, Austin, TX 78714. Questions? Call |
|
Refer to Attached Code Sheet for Numbered Fields |
|
*=These fields are required on all additional sheets submitted for this crash (ex.: additional vehicles, occupants, injured, etc.). |
Page of |
|
IDENTIFICATION & LOCATION
|
*Crash Date |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
*Crash Time |
|
|
|
|
|
|
|
|
|
|
Case |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(24HRMM) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
(MM/DD/YYYY) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ID |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
*County |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
*City |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
In your opinion, did this crash result in at least |
|
|
Yes |
Latitude |
|
|
|
|
|
. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Longitude |
|
|
|
|||||||||||||||||||||||||||||||||
|
$1,000 damage to any one person's property? |
|
|
No |
(decimal degrees) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(decimal degrees) |
|
||||||||||||||||||||||||||||||
|
ROAD ON WHICH CRASH OCCURRED |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
*1 Rdwy. |
|
|
|
|
|
|
*Hwy. |
|
|
|
|
|
2 Rdwy. |
|
|
|
|
|
|
Block |
|
|
|
|
|
|
|
|
|
|
|
|
|
3 Street |
|
|
|
|
|
|
|
|
* Street |
|
||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||
|
Sys. |
|
|
|
|
|
|
|
|
|
Num. |
|
|
|
|
|
Part |
|
|
|
|
|
|
|
Num. |
|
|
|
|
|
|
|
|
|
|
|
|
|
Prefix |
|
|
|
|
|
|
|
|
Name |
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Yes |
|
|
|
|
|
Yes |
|
|
Street |
|
||||||||||||||||||||||||||||||||
|
Crash Occurred on a Privat e Drive or |
|
Toll Road/ |
|
Speed |
|
|
|
|
|
|
|
|
|
Const . |
|
|
|
Workers |
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||||||
|
Road/ Privat e Propert y/ Parking Lot |
|
|
|
Toll Lane |
|
|
|
|
|
|
|
|
|
|
Zone |
|
|
|
|
|
|
Present |
|
|
|
|
|
|
|
|
|
Desc. |
|
|||||||||||||||||||||||||||||||||||||
|
|
|
|
|
Limit |
|
|
|
|
|
|
|
|
|
|
|
|
No |
|
|
|
|
No |
|
|
|
|||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
INTERSECTING ROAD, OR IF CRASH NOT AT INTERSECTION, NEAREST INTERSECTING ROAD OR REFERENCE M ARKER |
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||
|
At |
Yes |
1 Rdwy. |
Hwy. |
|
|
|
|
|
2. Rdwy. |
Block |
|
3 Street |
|
|
|
|
|
|
Street |
|
||||||||||||||||||||||||||||||||||||||||||||||||||
|
Int . |
No |
Sys. |
|
|
|
|
|
Num. |
|
|
|
|
|
Part |
Num. |
|
Prefix |
|
|
|
|
|
|
|
|
|
|
|
Name |
|
||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
FT |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Distance from Int. |
|
|
|
|
|
|
|
|
3 Dir. from Int. |
|
|
Reference |
|
|
|
|
Street |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||
|
or Ref. Marker |
|
|
|
|
|
|
|
|
|
|
|
MI |
|
or Ref. Marker |
|
|
Marker |
|
|
|
|
Desc. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||
|
Unit |
|
|
|
|
5 Unit |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
LP |
|
|
|
LP |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
Parked |
|
|
|
Hit and |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
VIN |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||
|
Num. |
|
|
|
|
Desc. |
|
|
|
|
|
Vehicle |
|
|
|
Run |
|
|
|
State |
|
|
|
Num. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||
|
Veh. |
|
|
|
|
|
|
|
|
|
|
6. Veh. |
|
|
|
|
|
|
|
|
|
Veh. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Veh. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
Year |
|
|
|
|
|
|
|
|
|
|
|
|
Color |
|
|
|
|
|
|
|
|
|
Make |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Model |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
8 DL/ID |
|
|
|
|
|
|
|
DL/ID |
|
|
DL/ID |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
9 DL |
|
10 CDL |
|
|
|
|
|
|
11 DL |
|
|||||||||||||||||||||||||||||||||
|
Type |
|
|
|
|
|
|
|
State |
|
|
Num. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Class |
|
End. |
|
|
|
|
|
|
|
|
|
|
|
Rest. |
|
||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Address (Street,
City, State, ZIP)
Local Use
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Out side |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Cit y Lim it |
|||
|
|
|
|
|
|
. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4 Street |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Suffix |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4 Street |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Suffix |
|||||||||
|
|
|
|
|
|
|
RRX |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
Num. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
7 Body |
|
|
|
|
|
|
|
|
|
|
Pol., Fire, EMS on |
|||||||||||
|
|
Style |
|
|
|
|
|
|
|
|
|
|
Em ergency (Explain in |
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
Narrat ive if checked) |
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
DOB |
/ |
/ |
|
|
|
|
|
|
|
|
||||||||||||||
(MM/DD/YYYY) |
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PERSONS Person .Num |
Prsn12. Type |
Seat13 |
ionPosit |
|
|
|
|
|
|
|
|
Nam e: Last , First , Middle |
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
Ent er Driver or Prim ary Person for t his Unit on first line |
|||||||||||
VEHICLE, DRIVER, & |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Owner |
|
Owner/Lessee |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
Lessee |
|
Name & Address |
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Proof of |
Yes |
Expired |
26 Fin. |
|
Fin. Resp. |
|
|
|
|
|
|||||||||||
|
Fin. Resp . |
No |
|
|
|
Exempt |
Resp. Type |
|
Name |
|
|
|
|
|
||||||||
|
Fin. Resp. |
|
|
|
|
|
|
|
|
|
|
|
|
|
27 Vehicle |
- |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
Phone Num. |
|
|
|
|
|
|
|
|
|
|
|
|
Damage Rating 1 |
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Towed |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Towed |
|
|
|
|
|
|
By |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
To |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Unit |
|
|
5 Unit |
|
|
|
|
Parked |
|
Hit and |
|
LP |
|
LP |
|||||||
|
Num. |
|
|
Desc. |
|
|
|
|
Vehicle |
|
Run |
|
State |
|
Num. |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Veh. |
|
|
|
|
|
|
|
6. Veh. |
|
|
Veh. |
|
|
|
|
|
|||||
|
Year |
|
|
|
|
|
|
|
Color |
|
|
Make |
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
8 DL/ID |
|
|
|
|
DL/ID |
|
|
DL/ID |
|
|
|
|
|
|
9 DL |
||||||
|
Type |
|
|
|
|
|
State |
|
|
Num. |
|
|
|
|
|
|
Class |
|||||
|
Address (Street, |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
City, State, ZIP) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
14 Injury |
|
Severit y |
|
Age |
15 Et hnicit y |
16 Sex |
|
17 Eject . |
|
18 Rest r. |
|
19 Airbag |
20 Helm et |
|
21 Sol. |
22 Alc. |
Spec. |
|
Alc. Result |
|
23 Drug Spec. |
24 Drug Result |
25 Drug Cat egory |
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Not Applicable - Alcohol and |
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Drug Result s are only report ed |
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
for Driver/ Prim ary Person for |
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
each Unit . |
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Fin. Resp. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
Num. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
- |
|
|
|
27 Vehicle |
|
|
|
|
|
|
|
|
- |
|
|
|
|
|
|
|
|
|
|
|
|
- |
|
|
|
|
Vehicle |
|
|
|
Yes |
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||
|
|
|
Damage Rating 2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Invent oried |
No |
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
VIN |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Veh. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
7 Body |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Pol., Fire, EMS on |
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Em ergency (Explain in |
||||||||||||||||||
|
|
Model |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Style |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Narrat ive if checked) |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
10 CDL |
|
|
|
|
|
11 DL |
|
|
|
|
|
|
|
DOB |
|
|
|
|
|
|
|
|
/ |
|
|
|
|
|
|
|
/ |
|
|
|
|
|
|
|
|
|
||||||||||
End. |
|
|
|
|
|
Rest. |
|
|
|
|
|
|
|
(MM/DD/YYYY) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PERSONS Person .Num |
Prsn12. Type |
Seat13 ionPosit |
|
|
|
Nam e: Last , First , Middle |
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
Ent er Driver or Prim ary Person for t his Unit on first line |
|||||||||||
VEHICLE, DRIVER, & |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Owner |
Owner/Lessee |
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Lessee |
Name & Address |
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
Expired |
|
26 Fin. |
|
Fin. Resp. |
|
|
|
|
|
|||||
|
Proof of |
Yes |
|
|
|
|
|
|
|
||||||||
|
Fin. Resp . |
No |
Exempt |
|
Resp. Type |
|
Name |
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Fin. Resp. |
|
|
|
|
|
|
27 Vehicle |
- |
|
|
|
|
||||
|
Phone Num. |
|
|
|
|
|
|
Damage Rating 1 |
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Towed |
|
|
|
|
|
|
|
|
Towed |
|
|
|
|
|
||
|
By |
|
|
|
|
|
|
|
|
To |
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
14 Injury Severit y |
Age |
15 Et hnicit y |
16 Sex |
17 Eject . |
18 Rest r. |
19 Airbag |
20 Helm et |
21 Sol. |
22 Alc. Spec. |
Alc. Result |
23 Drug Spec. |
24 Drug Result |
25 Drug Cat egory |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Not Applicable - Alcohol and Drug Result s are only report ed for Driver/ Prim ary Person for each Unit .
Fin. Resp.
Num.
- |
|
27 Vehicle |
- |
|
|
|
- |
|
Vehicle |
Yes |
||
|
|
|
|
|
|
|||||||
|
Damage Rating 2 |
|
|
|
|
|
|
Invent oried |
No |
|||
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
Sh ow Cod e Sh e e t f or N u m b e r e d Fie ld s
Law Enforcement and TxDOT Use ONLY. |
Case |
TxDOT |
|
|
|
Page |
of |
|
|||||||||
Form |
(Rev. 1/1/2018) |
ID |
Crash ID |
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Unit |
|
Prsn. |
|
Taken To |
|
Taken By |
Date of Death |
Time of Death |
|
|||||||
|
Num. |
|
Num. |
|
|
(MM/DD/YYYY) |
(24HR:MM) |
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
||||||||
DISPOSITION OF INJURED/ KILLED |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CHARGES
Unit Prsn. Num. Num.
Charge
Citation/Reference Num.
DAM AGE |
|
|
|
|
Damaged Property Other Than Vehicles |
|
|
|
|
|
|
|
|
|
|
Owner's Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Owner's Address |
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Unit |
|
|
|
|
|
|
10,001+ |
|
|
|
|
TRANSPORTING |
9+ CAPACITY |
|
CMV Disabling |
Yes |
|
28 Veh. |
|
|
|
29 Carrier |
|
|
|
|
|
Carrier |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||||||||
|
Num. |
|
|
|
|
|
LBS. |
|
|
HAZARDOUS MATERIAL |
|
Damage? |
|
|
No |
|
Oper. |
|
|
|
ID Type |
|
|
|
|
|
ID Num. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Carrier's |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Carrier's |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
30 |
|
|
|
|
|||||||
|
Corp. Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Primary Addr. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Veh.Typ |
|
|
|||||||||
V |
31 Bus |
|
|
|
|
|
|
RGVW |
|
|
|
|
|
|
|
|
|
|
HazMat |
Yes |
32 HazMat |
|
HazMat |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
32 HazMat |
HazMat |
|
|
|
|
|
|
|
|
|
|
|
|
|
33 Cargo |
|
|
|||||||||||||||||||||||||||||||||||
CM |
Type |
|
|
|
|
|
|
GVWR |
|
|
|
|
|
|
|
|
|
|
|
|
Released |
No |
Class Num. |
|
ID Num. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Class Num. |
|
|
ID Num. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Body Type |
|
|
|||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Unit |
|
|
|
|
|
|
|
|
RGVW |
|
|
|
|
|
|
|
|
|
|
|
34 Trlr. |
|
|
|
|
CMV Disabling |
Yes |
Unit |
|
|
|
|
|
|
|
|
|
|
RGVW |
|
|
|
|
|
|
|
|
|
|
34 Trlr. |
|
|
|
|
|
|
CMV Disabling |
Yes |
|||||||||||||||||||||||||||||||
|
Num. |
|
|
|
|
|
|
GVWR |
|
|
|
|
|
|
|
|
|
|
|
|
Type |
|
|
|
|
Damage? |
|
|
|
No |
Num. |
|
|
|
GVWR |
|
|
|
|
|
|
|
|
|
|
|
|
Type |
|
|
|
|
|
|
Damage? |
No |
||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Sequence |
35 Seq. 1 |
35 Seq. 2 |
35 Seq. 3 |
|
|
|
|
35 Seq. 4 |
|
|
|
|
|
|
|
|
Intermodal Shipping |
|
|
Yes |
Actual |
|
|
|
|
|
|
|
|
|
|
|
|
|
Total Num. |
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Of Events |
|
|
|
|
|
|
|
|
|
|
|
|
Container Permit |
|
|
No |
Gross |
|
|
|
|
|
|
|
|
|
|
|
|
|
Axles: |
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Weight |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||
|
CONDITIONS |
|
36 |
Contributing Factors |
(Investigator's Opinion) |
|
|
|
37 Vehicle Defects (Investigator's Opinion) |
|
|
|
|
|
|
|
|
|
|
|
Environmental and Roadway Conditions |
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
FACTORS& |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Unit # |
|
|
|
|
|
|
|
Contributing |
|
|
|
|
|
|
|
May Have Contrib. |
|
|
|
|
Contributing |
|
|
|
|
May Have Contrib. |
|
38 |
|
|
|
39 |
|
40 |
41 |
|
|
42 |
|
|
43 |
|
|
44 |
|||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Weather |
|
|
Light |
|
Entering |
Roadway |
Roadway |
|
Surface |
|
Traffic |
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Cond. |
|
|
Cond. |
|
|
Roads |
|
Type |
Alignment |
Condition |
|
Control |
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
Investigator's Narrative Opinion of What Happened |
|
|
|
|
|
|
|
|
|
|
Indicat e |
|
|
|
|
|
|
|
|
|
|
|
Field Diagram - Not t o Scale |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(Attach Additional Sheets if Necessary) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Nort h |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
NARRATIVE AND DIAGRAM |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||
INVESTIGATOR |
Time Notified |
|
|
|
|
|
|
|
|
|
|
How |
|
|
|
|
|
|
|
|
|
|
Time Arrived |
|
|
|
|
|
|
|
|
|
Report Date |
|
gion/DA |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||
Num. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
*Agency |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
(24HR:MM) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Notified |
|
|
|
|
|
|
|
|
|
|
(24HRMM) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(MM/DD/YYYY) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||
|
Invest. |
Yes |
|
Investigator |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ID |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
Comp. |
No |
|
Name (Printed) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Num. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
ORI |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Service/Re |
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Cont act / Help
Law Enforcement and TxDOT Use ONLY. |
Case |
|
|
|
|
TxDOT |
||||||||||||||||||
Form |
ID |
|
|
|
|
Crash ID |
||||||||||||||||||
|
* Crash Date |
|
|
|
|
|
|
|
|
|
|
|
|
*Crash Time |
|
|
|
|
|
*County |
||||
|
(MM/DD/YYYY) |
|
|
|
|
|
|
|
|
|
|
|
(24HRMM) |
|
|
|
|
|
Name |
|||||
|
* City |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
* 1 Rdwy. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Sys. |
|
|
* Street |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ORI |
|
|
|
|
|
|
|
|
|
|
|
|
|
*Agency |
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
Num. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Unit Num |
|
Person Num . |
12 Prsn. Type |
|
13 Seat Posit ion |
|
|
|
|
|
|
|
|
|
Nam e: Last , First , Middle |
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
Page of
*Hwy.
Num.
Service/Re
gion/DA
14 Injury Severit y |
Age |
15 Et hnicit y |
16 Sex |
17 Eject . |
18 Rest r. |
19 Airbag |
20 Helm et |
21 Sol. |
ADDITIONAL PERSONS
Law Enforcement and TxDOT Use ONLY. |
Case |
TxDOT |
|
|
||||||||||||
Form |
ID |
Crash ID |
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
*County |
|
|
|
|
* Crash Date |
|
*Crash Time |
|
|
|
||||||||||
|
(MM/DD/YYYY) |
|
(24HRMM) |
|
|
|
|
|
|
|
|
|
Name |
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
* City |
|
|
|
|
|
|
|
|
|
|
|
|
* 1 Rdwy. |
|
* Hwy. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Name |
|
|
|
|
|
|
|
|
|
|
|
|
Sys. |
|
Num. |
|
* Street |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Page of
ORI
Num.
Unit |
Prsn. |
Num . |
Num . |
|
|
DISPOSITION OFADDITIONAL INJURED/ KILLED
|
*Agency |
|
|
Service/Re |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
gion/DA |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Taken To |
Taken By |
Dat e of Deat h |
|
|
Tim e of Deat h |
||||
(MM/ DD/ YYYY) |
|
|
(24HRMM) |
||||||
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|