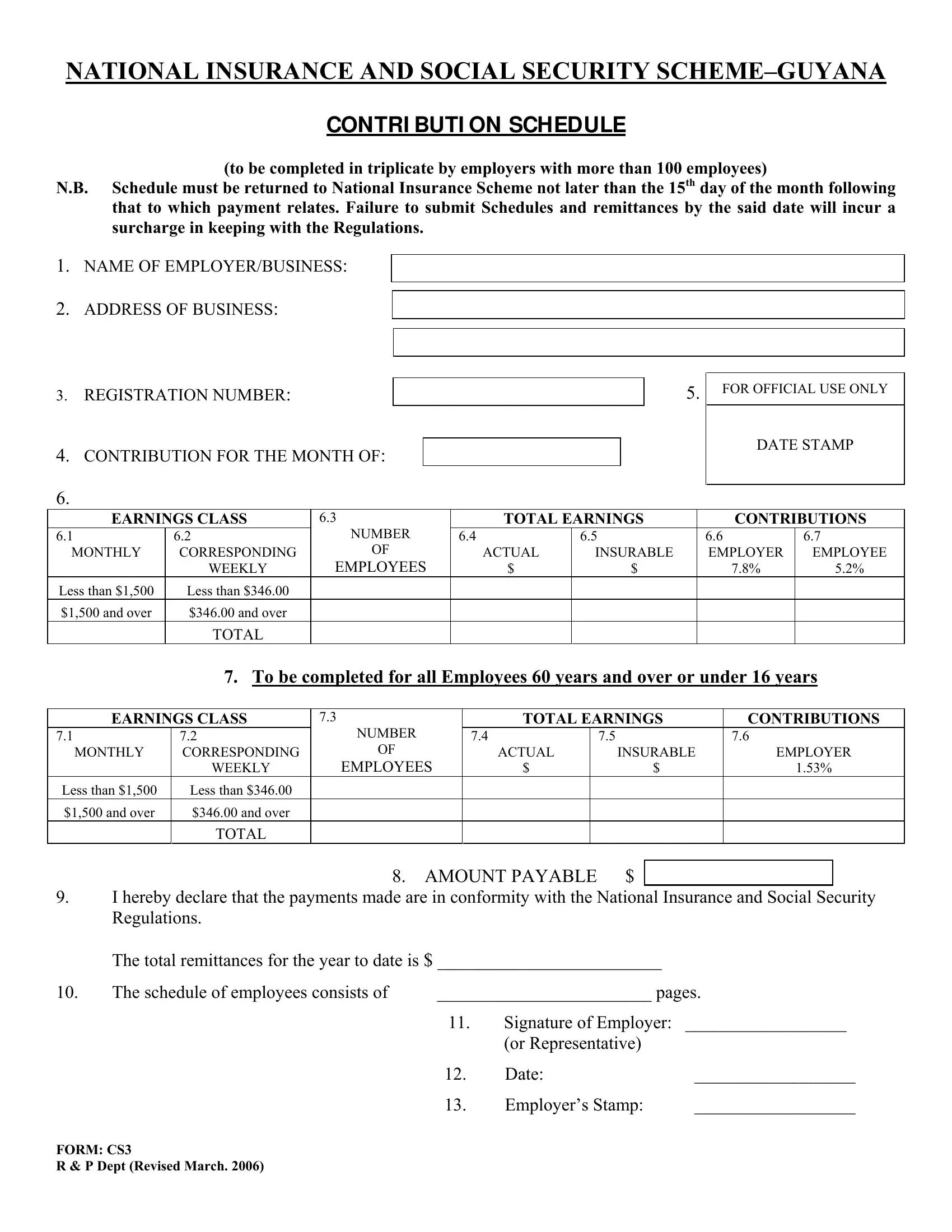
In the realm of the Guyanese workforce, adherence to national guidelines surrounding insurance and social security contributions is paramount for both employers and employees. The Contributions Schedule, commonly referred to by its form number CS3, stands out as a critical document for businesses with a workforce exceeding 100 individuals. This meticulously designed form acts as a conduit for employers to report and remit their employees' contributions to the National Insurance Scheme (NIS). Functioning under a strict deadline, the form mandates submission by no later than the 15th day of the month following the payment period. The CS3 form encompasses detailed sections requiring input on employer details, business address, registration number, and specific contribution amounts for each employee. Additionally, the form differentiates contributions rates based on the employee's earnings, dividing them into categories for those earning above or below set thresholds, and includes special considerations for employees who are either 60 years and older or under 16 years. A significant emphasis is also placed on the prompt and accurate completion of the form, underscoring the potential for incurable surcharges due to late submissions, as stipulated by the National Insurance and Social Security Regulations. The comprehensive design of the CS3 form underscores its role as not just a financial document, but a testament to the adherence to national regulations, ensuring the welfare of the broader workforce in Guyana.
| Question | Answer |
|---|---|
| Form Name | Form Cs3 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | incur, 15th, nis contribution schedule form cs3 forms, INSURABLE |
NATIONAL INSURANCE AND SOCIAL SECURITY
CONTRI BUTI ON SCHEDULE
(to be completed in triplicate by employers with more than 100 employees)
N.B. Schedule must be returned to National Insurance Scheme not later than the 15th day of the month following that to which payment relates. Failure to submit Schedules and remittances by the said date will incur a surcharge in keeping with the Regulations.
1.NAME OF EMPLOYER/BUSINESS:
2.ADDRESS OF BUSINESS:
3.REGISTRATION NUMBER:
4.CONTRIBUTION FOR THE MONTH OF:
5.
FOR OFFICIAL USE ONLY
DATE STAMP
6.
EARNINGS CLASS |
6.3 |
TOTAL EARNINGS |
CONTRIBUTIONS |
|||
6.1 |
6.2 |
NUMBER |
6.4 |
6.5 |
6.6 |
6.7 |
MONTHLY |
CORRESPONDING |
OF |
ACTUAL |
INSURABLE |
EMPLOYER |
EMPLOYEE |
|
WEEKLY |
EMPLOYEES |
$ |
$ |
7.8% |
5.2% |
Less than $1,500 |
Less than $346.00 |
|
|
|
|
|
$1,500 and over |
$346.00 and over |
|
|
|
|
|
|
TOTAL |
|
|
|
|
|
7.To be completed for all Employees 60 years and over or under 16 years
EARNINGS CLASS |
7.3 |
|
|
TOTAL EARNINGS |
CONTRIBUTIONS |
|||||
7.1 |
7.2 |
NUMBER |
|
7.4 |
|
|
7.5 |
|
7.6 |
|
MONTHLY |
CORRESPONDING |
OF |
|
|
ACTUAL |
|
INSURABLE |
EMPLOYER |
||
|
WEEKLY |
EMPLOYEES |
|
$ |
|
$ |
1.53% |
|
||
Less than $1,500 |
Less than $346.00 |
|
|
|
|
|
|
|
|
|
$1,500 and over |
$346.00 and over |
|
|
|
|
|
|
|
|
|
|
TOTAL |
|
|
|
|
|
|
|
|
|
|
|
8. |
AMOUNT PAYABLE |
$ |
|
|
|
|||
|
|
|
|
|
||||||
9.I hereby declare that the payments made are in conformity with the National Insurance and Social Security Regulations.
|
The total remittances for the year to date is $ ________________________ |
|
||
10. |
The schedule of employees consists of |
________________________ pages. |
||
|
|
11. |
Signature of Employer: |
__________________ |
|
|
|
(or Representative) |
|
|
|
12. |
Date: |
__________________ |
|
|
13. |
Employer’s Stamp: |
__________________ |
FORM: CS3
R & P Dept (Revised March. 2006)