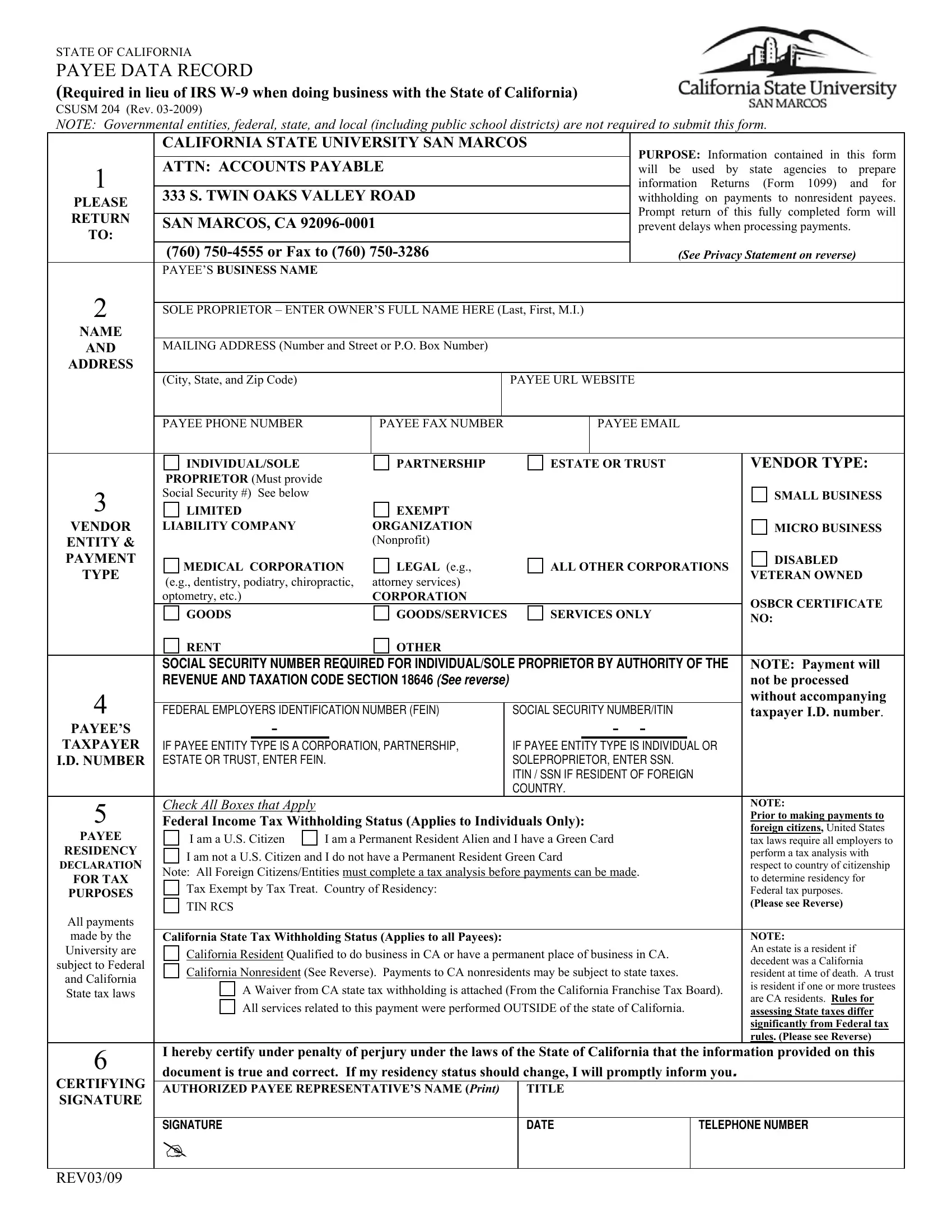
CSUSM 204 (Rev. 03-2009)
NOTE: Governmental entities, federal, state, and local (including public school districts) are not required to submit this form.
|
CALIFORNIA STATE UNIVERSITY SAN MARCOS |
PURPOSE: Information contained in this form |
|
|
|
|
|
|
|
|
|
|
|
|
ATTN: ACCOUNTS PAYABLE |
|
|
|
|
1 |
|
|
|
|
will be used by state agencies to prepare |
|
|
|
|
|
|
|
|
|
|
information Returns (Form 1099) and for |
333 S. TWIN OAKS VALLEY ROAD |
|
|
|
|
PLEASE |
|
|
|
|
withholding |
on payments to |
nonresident payees. |
|
|
|
|
|
|
|
|
|
|
Prompt return of |
this fully |
completed form will |
RETURN |
|
|
|
|
|
|
|
|
|
|
SAN MARCOS, CA 92096-0001 |
|
|
|
|
|
|
|
|
prevent delays when processing payments. |
TO: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(760) 750-4555 or Fax to (760) 750-3286 |
|
|
|
|
(See Privacy Statement on reverse) |
|
PAYEE’S BUSINESS NAME |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SOLE PROPRIETOR – ENTER OWNER’S FULL NAME HERE (Last, First, M.I.) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
NAME |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
AND |
MAILING ADDRESS (Number and Street or P.O. Box Number) |
|
|
|
|
|
|
|
|
|
|
|
ADDRESS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(City, State, and Zip Code) |
|
|
|
|
PAYEE URL WEBSITE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PAYEE PHONE NUMBER |
|
|
PAYEE FAX NUMBER |
|
|
|
PAYEE EMAIL |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
INDIVIDUAL/SOLE |
|
|
PARTNERSHIP |
|
ESTATE OR TRUST |
|
|
VENDOR TYPE: |
|
PROPRIETOR (Must provide |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3 |
Social Security #) See below |
|
|
|
|
|
|
|
|
|
|
|
|
|
SMALL BUSINESS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
LIMITED |
|
|
EXEMPT |
|
|
|
|
|
|
|
|
|
|
|
VENDOR |
LIABILITY COMPANY |
|
|
ORGANIZATION |
|
|
|
|
|
|
|
|
|
MICRO BUSINESS |
ENTITY & |
|
|
|
|
(Nonprofit) |
|
|
|
|
|
|
|
|
|
|
|
PAYMENT |
MEDICAL CORPORATION |
LEGAL (e.g., |
|
ALL OTHER CORPORATIONS |
|
DISABLED |
TYPE |
|
|
VETERAN OWNED |
(e.g., dentistry, podiatry, chiropractic, |
attorney services) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
optometry, etc.) |
|
|
CORPORATION |
|
|
|
|
|
|
|
|
|
OSBCR CERTIFICATE |
|
GOODS |
|
|
GOODS/SERVICES |
|
SERVICES ONLY |
|
|
|
|
|
|
|
|
NO: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
RENT |
|
|
OTHER |
|
|
|
|
|
|
|
|
|
|
|
|
SOCIAL SECURITY NUMBER REQUIRED FOR INDIVIDUAL/SOLE PROPRIETOR BY AUTHORITY OF THE |
|
NOTE: Payment will |
|
REVENUE AND TAXATION CODE SECTION 18646 (SEE REVERSE) |
|
|
|
|
|
|
|
|
|
not be processed |
4 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
without accompanying |
FEDERAL EMPLOYERS IDENTIFICATION NUMBER (FEIN) |
|
SOCIAL SECURITY NUMBER/ITIN |
|
|
taxpayer I.D. number. |
PAYEE’S |
|
- |
|
|
|
|
|
- - |
|
|
|
|
|
|
TAXPAYER |
IF PAYEE ENTITY TYPE IS A CORPORATION, PARTNERSHIP, |
|
IF PAYEE ENTITY TYPE IS INDIVIDUAL OR |
|
|
|
I.D. NUMBER |
ESTATE OR TRUST, ENTER FEIN. |
|
|
SOLEPROPRIETOR, ENTER SSN. |
|
|
|
|
|
|
|
|
|
|
|
ITIN / SSN IF RESIDENT OF FOREIGN |
|
|
|
|
|
|
|
|
|
|
|
COUNTRY. |
|
|
|
|
5 |
Check All Boxes that Apply |
|
|
|
|
|
|
|
|
|
|
|
|
|
NOTE: |
|
Federal Income Tax Withholding Status (Applies to Individuals Only): |
|
|
Prior to making payments to |
|
|
foreign citizens, United States |
PAYEE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
I am a U.S. Citizen |
I am a Permanent Resident Alien and I have a Green Card |
|
|
tax laws require all employers to |
RESIDENCY |
I am not a U.S. Citizen and I do not have a Permanent Resident Green Card |
|
|
perform a tax analysis with |
DECLARATION |
|
|
respect to country of citizenship |
Note: All Foreign Citizens/Entities must complete a tax analysis before payments can be made. |
|
|
FOR TAX |
|
|
to determine residency for |
Tax Exempt by Tax Treat. Country of Residency: |
|
|
|
|
|
|
|
|
|
PURPOSES |
|
|
|
|
|
|
|
|
|
Federal tax purposes. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(Please see Reverse) |
|
TIN RCS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
All payments |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
made by the |
California State Tax Withholding Status (Applies to all Payees): |
|
|
|
|
|
|
|
|
|
NOTE: |
|
University are |
California Resident Qualified to do business in CA or have a permanent place of business in CA. |
|
|
An estate is a resident if |
subject to Federal |
|
|
decedent was a California |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
California Nonresident (See Reverse). Payments to CA nonresidents may be subject to state taxes. |
|
|
resident at time of death. A trust |
and California |
|
|
A Waiver from CA state tax withholding is attached (From the California Franchise Tax Board). |
|
is resident if one or more trustees |
State tax laws |
|
|
are CA residents. Rules for |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
All services related to this payment were performed OUTSIDE of the state of California. |
|
|
|
|
|
assessing State taxes differ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
significantly from Federal tax |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
rules. (Please see Reverse) |
6 |
I hereby certify under penalty of perjury under the laws of the State of California that the information provided on this |
document is true and correct. If my residency status should change, I will promptly inform you. |
|
CERTIFYING |
|
AUTHORIZED PAYEE REPRESENTATIVE’S NAME (Print) |
|
TITLE |
|
|
|
|
SIGNATURE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SIGNATURE |
|
|
|
|
|
DATE |
|
TELEPHONE NUMBER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|