
Using PDF files online is actually simple with our PDF tool. You can fill in discontinuance here effortlessly. The editor is constantly maintained by us, acquiring new awesome functions and becoming better. Starting is simple! All you should do is stick to the next simple steps directly below:
Step 1: Just click the "Get Form Button" at the top of this site to get into our pdf form editing tool. Here you will find everything that is necessary to fill out your document.
Step 2: Once you open the editor, you will find the form all set to be filled out. Apart from filling in different blank fields, it's also possible to perform some other things with the Document, namely writing your own textual content, changing the original text, adding illustrations or photos, affixing your signature to the document, and much more.
This PDF form will need you to provide specific details; to ensure consistency, please be sure to pay attention to the subsequent suggestions:
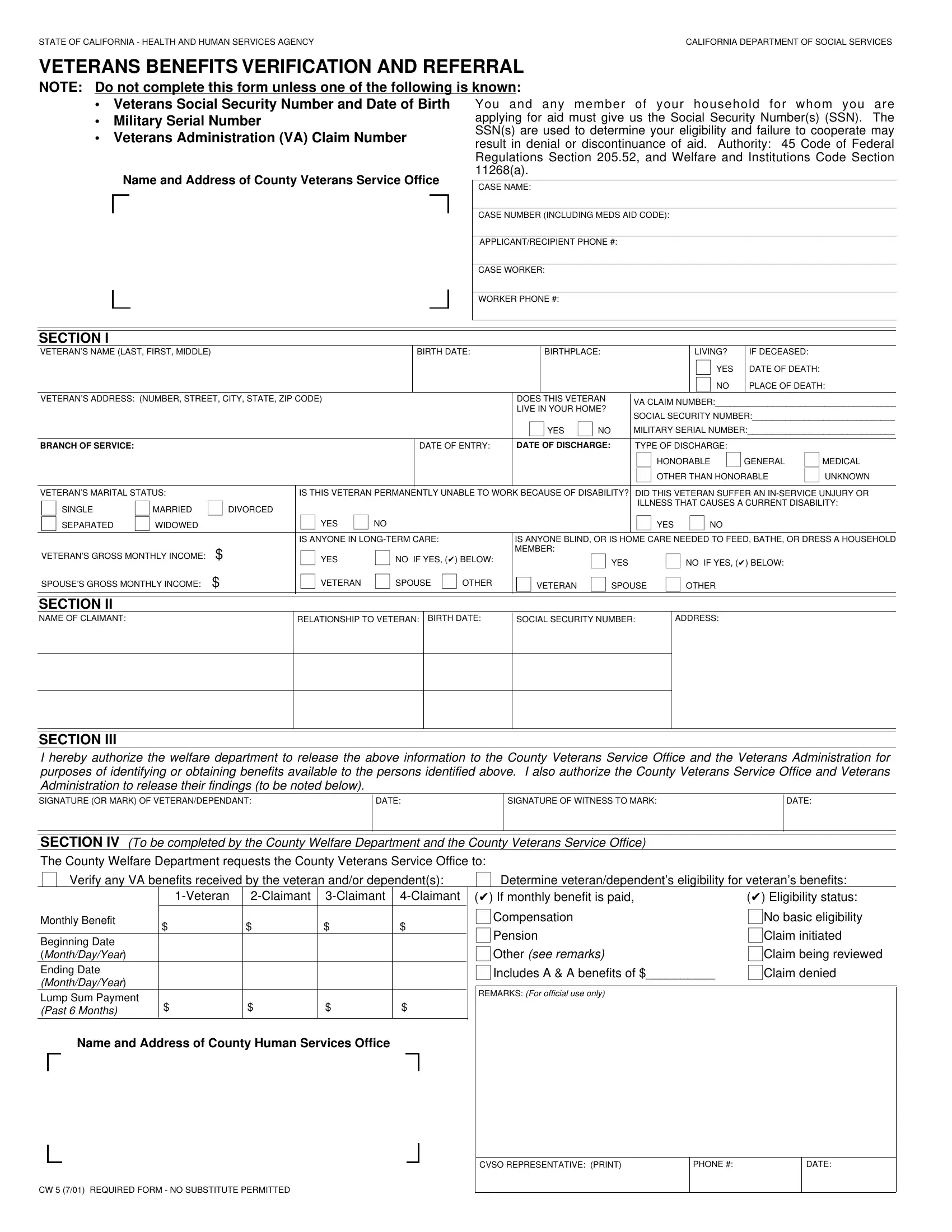
1. While filling out the discontinuance, ensure to complete all of the important fields within the relevant form section. This will help to expedite the work, enabling your information to be processed fast and properly.
2. Just after the last selection of blank fields is completed, go on to type in the suitable information in all these: SPOUSES GROSS MONTHLY INCOME, SECTION II NAME OF CLAIMANT, VETERAN, NO IF YES SPOUSE, OTHER, VETERAN, SPOUSE, OTHER, RELATIONSHIP TO VETERAN BIRTH DATE, SOCIAL SECURITY NUMBER, ADDRESS, SECTION III I hereby authorize the, SIGNATURE OF WITNESS TO MARK, DATE, and DATE.
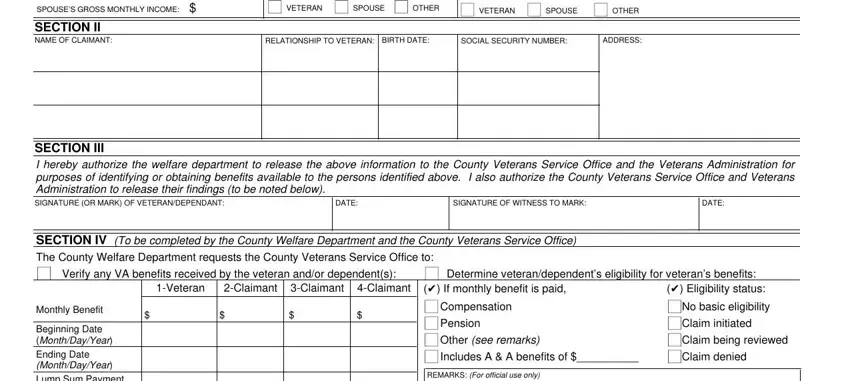
People frequently get some points incorrect while filling in SECTION II NAME OF CLAIMANT in this section. You should definitely revise everything you type in right here.
Step 3: Make certain the information is accurate and then simply click "Done" to continue further. Try a free trial option with us and gain immediate access to discontinuance - available in your FormsPal account page. Here at FormsPal, we aim to ensure that your information is maintained secure.