

Dealing with PDF forms online is definitely very simple with our PDF editor. Anyone can fill in california cw department social here without trouble. To maintain our tool on the cutting edge of practicality, we strive to implement user-driven features and improvements regularly. We are routinely looking for suggestions - join us in remolding the way you work with PDF docs. To get the process started, consider these simple steps:
Step 1: Click on the orange "Get Form" button above. It'll open up our pdf editor so that you could start completing your form.
Step 2: The editor offers you the ability to modify the majority of PDF forms in many different ways. Change it with customized text, adjust what's originally in the file, and put in a signature - all within several clicks!
It is straightforward to complete the form with this helpful guide! Here's what you need to do:
1. Fill out your california cw department social with a number of essential fields. Get all of the required information and make sure there's nothing overlooked!
2. Soon after completing this section, go on to the subsequent part and fill out the necessary particulars in all these blanks - Section I must be completed by the, Licensed physician or certified, SECTION PATIENTCLIENT INFORMATION, NAME OF PATIENTCLIENT LAST FIRST, SEX CIRCLE, BIRTH DATE, SOCIAL SECURITY NUMBER, AGES OF CHILDREN IN HOME, M F, I authorize of, NAME OF PROVIDER, CLINIC OR MEDICAL GROUP, to release information to the, Mental Condition, and Physical Condition.
3. Within this part, look at The information requested is, Questions through, Question, Question, Does the patient have a medically, from performing certain tasks, YES, Onset Date of Condition The, Chronic, Is the patient actively seeking, YES, Acute expected to last until NO, YES, Is this person able to work, and Does this person have any. All these will have to be taken care of with greatest accuracy.
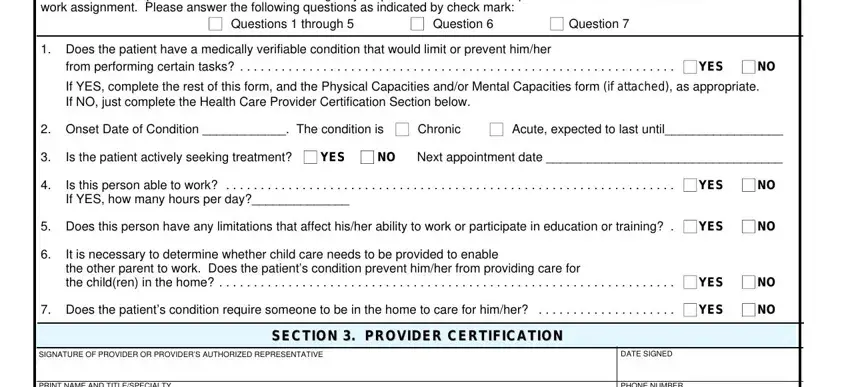
People who use this document often make some mistakes while completing Is the patient actively seeking in this part. You need to double-check everything you type in right here.
4. This next section requires some additional information. Ensure you complete all the necessary fields - PRINT NAME AND TITLESPECIALTY, STREET ADDRESS, MAILING ADDRESS IF DIFFERENT, CITY, CW REQUIRED FORM SUBSTITUTE, PHONE NUMBER, and STATE ZIP CODE - to proceed further in your process!

Step 3: Make sure your details are accurate and press "Done" to proceed further. Create a free trial option at FormsPal and acquire immediate access to california cw department social - download, email, or edit in your FormsPal account page. We do not share or sell the information you provide whenever dealing with forms at our site.