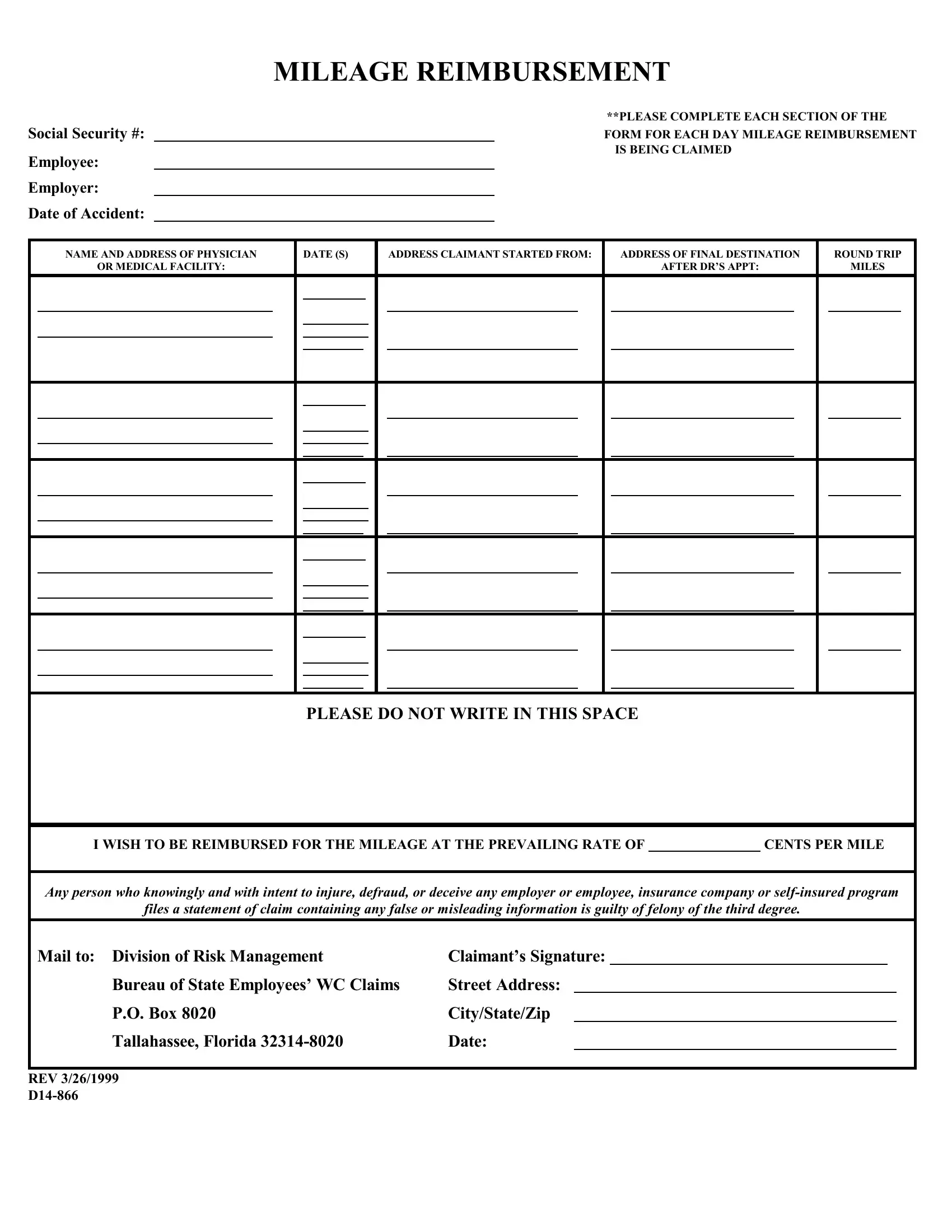
Understanding the logistics and provisions of the D14 866 form is crucial for employees seeking mileage reimbursement in the wake of an accident. This document, designed to facilitate compensation for travel expenses related to medical treatments or assessments, requires detailed information to ensure proper processing. It requests inputs such as Social Security number, employee and employer details, and the date of the accident, setting the stage for a request. The form meticulously requires the name and address of the physician visited, the date(s) of the visit(s), the starting address, and the final destination address, alongside the round trip miles covered. It emphasizes the necessity of completing each section for every day reimbursement is sought, underlining the meticulous nature of the claim process. Importantly, the document also warns against the submission of fraudulent claims, stating that false or misleading information could result in a third-degree felony charge. This stern warning serves as a deterrent against dishonesty, ensuring that the process remains fair and just. At the conclusion of the form, it guides claimants to direct their submissions to the Division of Risk Management, Bureau of State Employees’ WC Claims, providing a specific mailing address in Tallahassee, Florida. By laying out these requirements and instructions, the D14 866 form underpins the systematic approach to claiming mileage reimbursements, making it imperative for claimants to adhere to its stipulations meticulously.
| Question | Answer |
|---|---|
| Form Name | Form D14 866 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | rev 1 2017 d14 866, APPT, rev 7 2014 d14 866, rve d14 866 |
MILEAGE REIMBURSEMENT
Social Security #:
Employee:
Employer:
Date of Accident:
**PLEASE COMPLETE EACH SECTION OF THE
FORM FOR EACH DAY MILEAGE REIMBURSEMENT IS BEING CLAIMED
|
NAME AND ADDRESS OF PHYSICIAN |
|
DATE (S) |
|
ADDRESS CLAIMANT STARTED FROM: |
|
ADDRESS OF FINAL DESTINATION |
|
ROUND TRIP |
|||||||
|
OR MEDICAL FACILITY: |
|
|
|
|
|
|
|
|
|
AFTER DR’S APPT: |
|
MILES |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PLEASE DO NOT WRITE IN THIS SPACE |
|
|
|
|
|||
|
|
|
|
|
|
|
|
I WISH TO BE REIMBURSED FOR THE MILEAGE AT THE PREVAILING RATE OF |
|
CENTS PER MILE |
|||||
|
|
|
|
|
|
|
|
Any person who knowingly and with intent to injure, defraud, or deceive any employer or employee, insurance company or |
|||||||
files a statement of claim containing any false or misleading information is guilty of felony of the third degree. |
|||||||
Mail to: Division of Risk Management |
Claimant’s Signature: |
|
|
|
|
|
|
Bureau of State Employees’ WC Claims |
Street Address: |
|
|
|
|
|
|
P.O. Box 8020 |
City/State/Zip |
|
|
|
|
|
|
Tallahassee, Florida |
Date: |
|
|
|
|
|
|
REV 3/26/1999