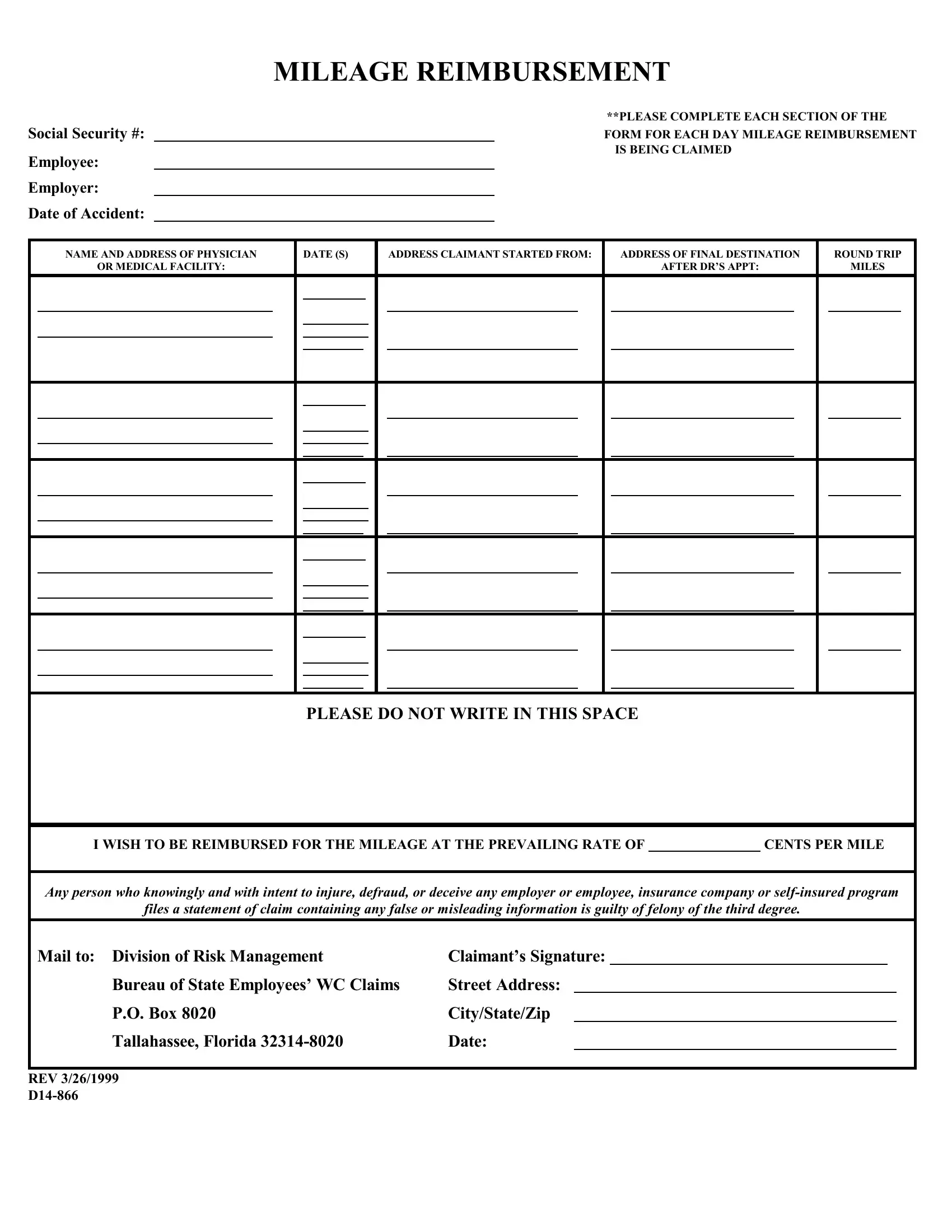
Form D14 866 is a tax form used to report the sale or exchange of certain capital assets. This form must be filed by the taxpayer within 30 days of the sale or exchange. The purpose of this form is to report the proceeds from the sale or exchange, as well as any related expenses. Failure to file this form may result in penalties and interest charges. taxpayers should always consult with a tax professional to ensure they are filing all required forms.
| Question | Answer |
|---|---|
| Form Name | Form D14 866 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | rev 1 2017 d14 866, APPT, rev 7 2014 d14 866, rve d14 866 |
MILEAGE REIMBURSEMENT
Social Security #:
Employee:
Employer:
Date of Accident:
**PLEASE COMPLETE EACH SECTION OF THE
FORM FOR EACH DAY MILEAGE REIMBURSEMENT IS BEING CLAIMED
|
NAME AND ADDRESS OF PHYSICIAN |
|
DATE (S) |
|
ADDRESS CLAIMANT STARTED FROM: |
|
ADDRESS OF FINAL DESTINATION |
|
ROUND TRIP |
|||||||
|
OR MEDICAL FACILITY: |
|
|
|
|
|
|
|
|
|
AFTER DR’S APPT: |
|
MILES |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PLEASE DO NOT WRITE IN THIS SPACE |
|
|
|
|
|||
|
|
|
|
|
|
|
|
I WISH TO BE REIMBURSED FOR THE MILEAGE AT THE PREVAILING RATE OF |
|
CENTS PER MILE |
|||||
|
|
|
|
|
|
|
|
Any person who knowingly and with intent to injure, defraud, or deceive any employer or employee, insurance company or |
|||||||
files a statement of claim containing any false or misleading information is guilty of felony of the third degree. |
|||||||
Mail to: Division of Risk Management |
Claimant’s Signature: |
|
|
|
|
|
|
Bureau of State Employees’ WC Claims |
Street Address: |
|
|
|
|
|
|
P.O. Box 8020 |
City/State/Zip |
|
|
|
|
|
|
Tallahassee, Florida |
Date: |
|
|
|
|
|
|
REV 3/26/1999