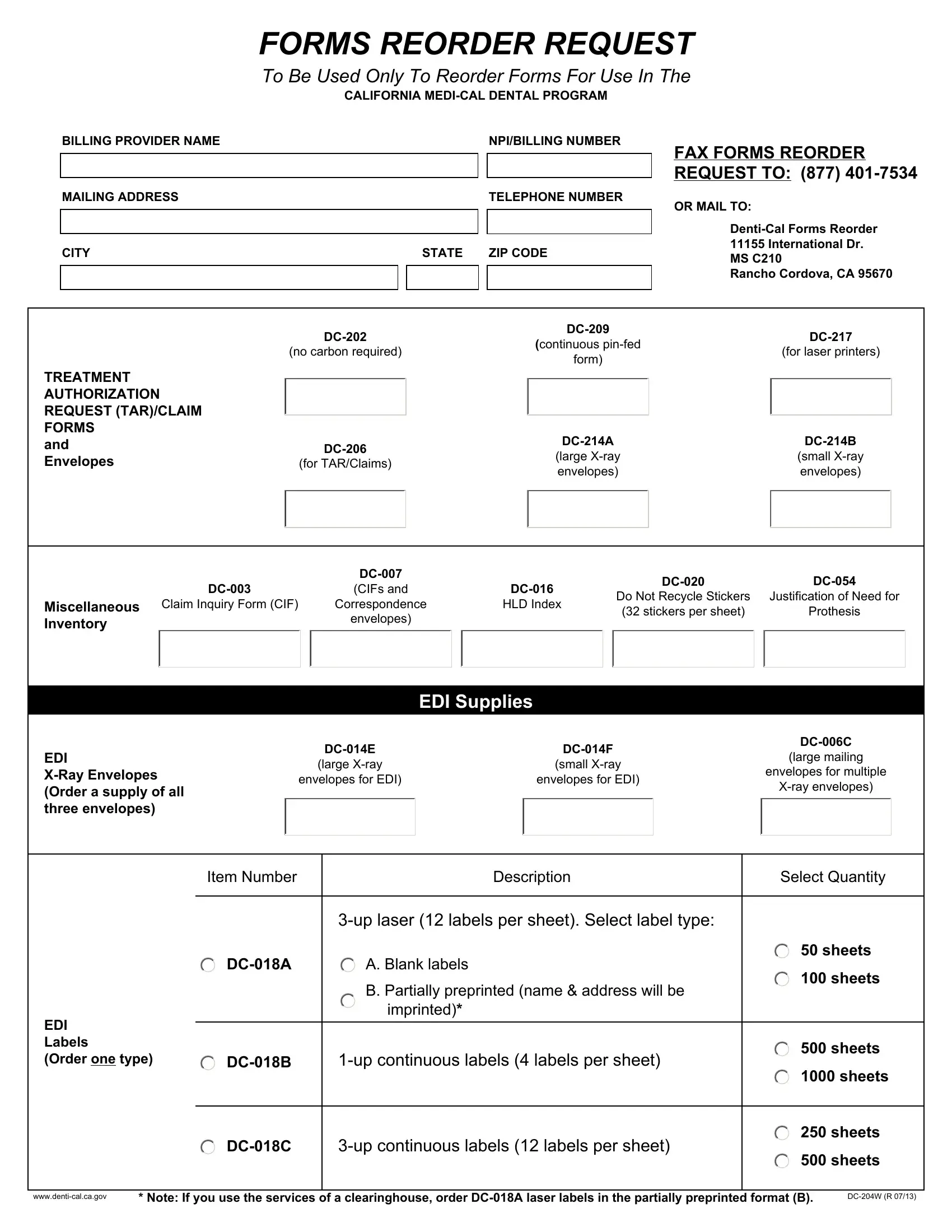
In the landscape of the California Medi-Cal Dental Program, the DC-204W form serves as a crucial tool for healthcare providers, ensuring they can smoothly reorder necessary forms essential for the execution of their administrative duties. This form streamlines the process of requesting various forms ranging from Treatment Authorization Request (TAR)/Claim forms to EDI labels, making it easier for providers to maintain a consistent supply of the documents crucial for patient care and billing processes. By meticulously specifying the types of forms available—for instance, continuous pin-fed forms, laser printer-compatible forms, and envelopes of varying sizes for X-rays or multiple documents—the form caters to the diverse needs within the dental care setting. Providers are required to indicate the quantity of each item needed, further simplifying the restocking process. Moreover, the form accommodates the selection between blank or partially preprinted labels, allowing for customization based on the provider's specific requirements. Facilities are directed to either fax or mail this form to a designated address, showcasing an effort to accommodate varying preferences for form submission. This adaptability underscores the form's importance in keeping dental care providers within the California Medi-Cal Dental Program well-equipped, ensuring they can focus more on delivering care and less on administrative hassles.
| Question | Answer |
|---|---|
| Form Name | Form Dc 204W |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | dc 054 form dentical, dc054 form denti cal, dc 054 denti cal, cd 054 form dentical |
|
FORMS REORDER REQUEST |
|||
|
To Be Used Only To Reorder Forms For Use In The |
|||
|
CALIFORNIA |
|||
BILLING PROVIDER NAME |
|
|
NPI/BILLING NUMBER |
|
|
|
|
|
FAX FORMS REORDER |
|
|
|
|
|
|
|
|
|
REQUEST TO: (877) |
|
|
|
|
|
MAILING ADDRESS |
|
|
TELEPHONE NUMBER |
|
|
|
|
|
|
|
|
|
|
|
CITY |
STATE ZIP CODE |
|||
|
|
|
|
|
|
|
|
|
|
OR MAIL TO:
11155 International Dr.
MS C210
Rancho Cordova, CA 95670
|
||||||
|
(continuous |
|||||
|
(no carbon required) |
(for laser printers) |
||||
|
form) |
|||||
|
|
|
|
|||
TREATMENT |
|
|
|
|
|
|
|
|
|
|
|
||
AUTHORIZATION |
|
|
|
|
|
|
REQUEST (TAR)/CLAIM |
|
|
|
|
|
|
FORMS |
|
|
|
|
|
|
and |
||||||
|
(large |
(small |
||||
Envelopes |
(for TAR/Claims) |
|||||
envelopes) |
envelopes) |
|||||
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
(CIFs and |
|
|
||||||
|
|
|
Do Not Recycle Stickers |
Justification of Need for |
|||||
Miscellaneous Claim Inquiry Form (CIF) |
Correspondence |
|
HLD Index |
|
|||||
|
|
(32 stickers per sheet) |
Prothesis |
||||||
|
|
|
envelopes) |
|
|
|
|||
Inventory |
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
EDI Supplies
EDI
|
||||
|
(large mailing |
|||
(large |
(small |
|
||
|
envelopes for multiple |
|||
envelopes for EDI) |
envelopes for EDI) |
|
||
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Item Number |
Description |
Select Quantity |
|
|
|
|
|
50 sheets |
|
A. Blank labels |
|
|
|
100 sheets |
|
|
B. Partially preprinted (name & address will be |
|
|
imprinted)* |
EDI |
|
|
|
|
|
Labels |
|
500 sheets |
|
|
|
(Order one type) |
||
|
|
1000 sheets |
250 sheets
500 sheets
* Note: If you use the services of a clearinghouse, order |