|
|
|
|
|
|
|
|
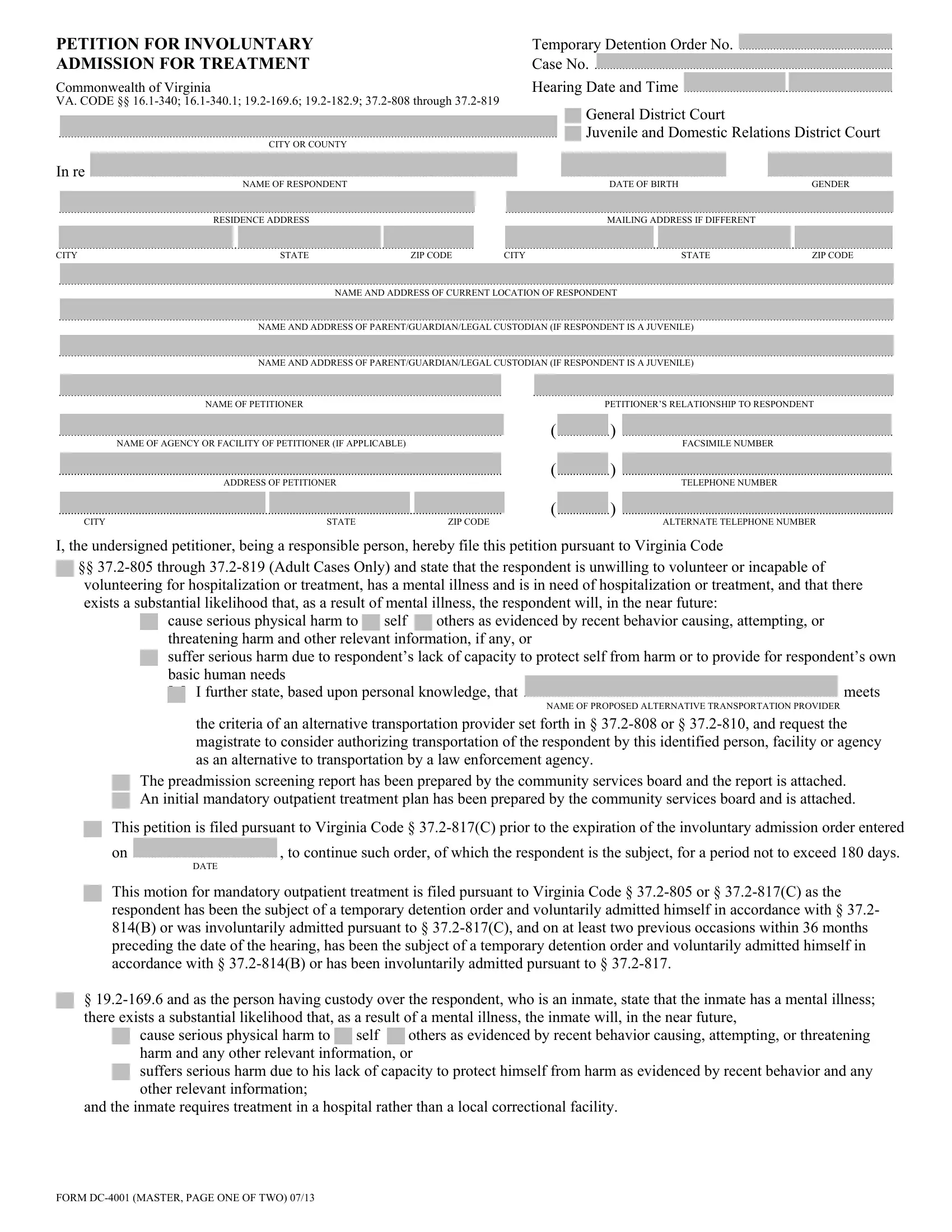
PETITION FOR INVOLUNTARY |
Temporary Detention Order No |
|
|
|
|
.................................................. |
|
ADMISSION FOR TREATMENT |
Case No |
|
|
|
|
|
|
|
|
|
|
Commonwealth of Virginia |
Hearing Date and Time |
|
|
|
|
|
|
VA. CODE §§ 16.1-340; 16.1-340.1; 19.2-169.6; 19.2-182.9; 37.2-808 through 37.2-819 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
[ |
] |
General District Court |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
.................................................................................................................................................................. |
|
|
|
|
|
|
|
|
|
|
|
|
[ |
] |
Juvenile and Domestic Relations District Court |
|
|
|
|
CITY OR COUNTY |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
In re |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
...................................................... |
|
......................................... |
|
|
NAME OF RESPONDENT |
|
|
|
|
|
|
|
|
GENDER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DATE OF BIRTH |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
....................................................................................................................................... |
|
|
|
|
|
|
|
|
.............................................................................................................................. |
|
|
RESIDENCE ADDRESS |
|
|
|
|
|
|
|
|
|
|
MAILING ADDRESS IF DIFFERENT |
|
|
....................................................................................................................................... |
|
|
|
|
|
|
|
.............................................................................................................................. |
|
|
|
|
|
|
|
|
CITY |
|
|
STATE |
|
ZIP CODE |
CITY |
|
STATE |
|
ZIP CODE |
...............................................................................................................................................................................................................................................................................
NAME AND ADDRESS OF CURRENT LOCATION OF RESPONDENT
...............................................................................................................................................................................................................................................................................
NAME AND ADDRESS OF PARENT/GUARDIAN/LEGAL CUSTODIAN (IF RESPONDENT IS A JUVENILE)
...............................................................................................................................................................................................................................................................................
NAME AND ADDRESS OF PARENT/GUARDIAN/LEGAL CUSTODIAN (IF RESPONDENT IS A JUVENILE)
................................................................................................................................................ .....................................................................................................................
NAME OF PETITIONERPETITIONER’S RELATIONSHIP TO RESPONDENT
|
|
|
|
|
|
|
( |
................. |
) |
|
|
................................................................................................................................................ |
|
|
|
|
|
|
........................................................................................ |
|
|
NAME OF AGENCY OR FACILITY OF PETITIONER (IF APPLICABLE) |
|
|
|
|
FACSIMILE NUMBER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
................. |
) |
|
|
................................................................................................................................................ |
|
|
|
|
( |
|
........................................................................................ |
|
|
ADDRESS OF PETITIONER |
|
|
|
TELEPHONE NUMBER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
( |
................. |
) |
|
|
................................................................................................................................................ |
|
|
|
|
|
........................................................................................ |
|
|
|
|
|
|
|
|
|
CITY |
|
|
STATE |
|
ZIP CODE |
|
|
ALTERNATE TELEPHONE NUMBER |
|
I, the undersigned petitioner, being a responsible person, hereby file this petition pursuant to Virginia Code
[] §§ 37.2-805 through 37.2-819 (Adult Cases Only) and state that the respondent is unwilling to volunteer or incapable of volunteering for hospitalization or treatment, has a mental illness and is in need of hospitalization or treatment, and that there exists a substantial likelihood that, as a result of mental illness, the respondent will, in the near future:
[ ] cause serious physical harm to [ ] self [ ] others as evidenced by recent behavior causing, attempting, or threatening harm and other relevant information, if any, or
[] suffer serious harm due to respondent’s lack of capacity to protect self from harm or to provide for respondent’s own basic human needs
[ ] |
I further state, based upon personal knowledge, that |
...................................................................................................... meets |
|
|
NAME OF PROPOSED ALTERNATIVE TRANSPORTATION PROVIDER |
the criteria of an alternative transportation provider set forth in § 37.2-808 or § 37.2-810, and request the magistrate to consider authorizing transportation of the respondent by this identified person, facility or agency as an alternative to transportation by a law enforcement agency.
[] The preadmission screening report has been prepared by the community services board and the report is attached.
[] An initial mandatory outpatient treatment plan has been prepared by the community services board and is attached.
[ ] This petition is filed pursuant to Virginia Code § 37.2-817(C) prior to the expiration of the involuntary admission order entered
|
|
|
on |
, to continue such order, of which the respondent is the subject, for a period not to exceed 180 days. |
|
DATE |
[] This motion for mandatory outpatient treatment is filed pursuant to Virginia Code § 37.2-805 or § 37.2-817(C) as the respondent has been the subject of a temporary detention order and voluntarily admitted himself in accordance with § 37.2- 814(B) or was involuntarily admitted pursuant to § 37.2-817(C), and on at least two previous occasions within 36 months preceding the date of the hearing, has been the subject of a temporary detention order and voluntarily admitted himself in accordance with § 37.2-814(B) or has been involuntarily admitted pursuant to § 37.2-817.
[] § 19.2-169.6 and as the person having custody over the respondent, who is an inmate, state that the inmate has a mental illness; there exists a substantial likelihood that, as a result of a mental illness, the inmate will, in the near future,
[ ] cause serious physical harm to [ ] self [ ] others as evidenced by recent behavior causing, attempting, or threatening harm and any other relevant information, or
[ ] suffers serious harm due to his lack of capacity to protect himself from harm as evidenced by recent behavior and any other relevant information;
and the inmate requires treatment in a hospital rather than a local correctional facility.
FORM DC-4001 (MASTER, PAGE ONE OF TWO) 07/13
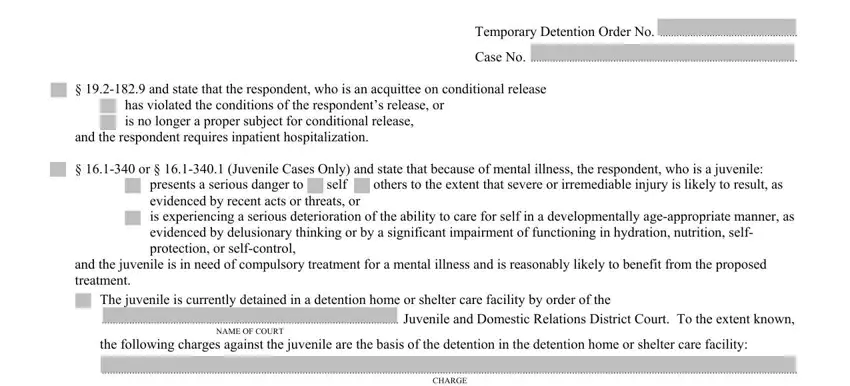
Temporary Detention Order No. ..................................................
Case No. .................................................................................................
[] § 19.2-182.9 and state that the respondent, who is an acquittee on conditional release [ ] has violated the conditions of the respondent’s release, or
[ ] is no longer a proper subject for conditional release,
and the respondent requires inpatient hospitalization.
[ ] § 16.1-340 or § 16.1-340.1 (Juvenile Cases Only) and state that because of mental illness, the respondent, who is a juvenile:
[ ] presents a serious danger to [ ] self [ ] others to the extent that severe or irremediable injury is likely to result, as evidenced by recent acts or threats, or
[] is experiencing a serious deterioration of the ability to care for self in a developmentally age-appropriate manner, as evidenced by delusionary thinking or by a significant impairment of functioning in hydration, nutrition, self-
protection, or self-control,
and the juvenile is in need of compulsory treatment for a mental illness and is reasonably likely to benefit from the proposed treatment.
[ ] The juvenile is currently detained in a detention home or shelter care facility by order of the
............................................................................................................ Juvenile and Domestic Relations District Court. To the extent known,
NAME OF COURT
the following charges against the juvenile are the basis of the detention in the detention home or shelter care facility:
.............................................................................................................................................................................................................................................................
CHARGE
.............................................................................................................................................................................................................................................................
CHARGE
[ ] See attached sheet for additional charges.
To the extent known, the names and addresses of the juvenile’s parents are as follows:
......................................................................................................................................................................................................................................................................
NAME OF MOTHER AND ADDRESS
......................................................................................................................................................................................................................................................................
NAME OF FATHER AND ADDRESS
I request that the respondent be examined and accorded such assistance as provided by law. In support of this petition, I further state
as follows:
........................................................................................................................................................................................................................................................
.......................................................................................... |
______________________________________________________________ |
|
DATE |
PETITIONER |
The petitioner appeared this date before the undersigned and, upon being duly sworn, made oath that the facts stated in this petition are true based on the petitioner’s knowledge.
..........................................................................................______________________________________________________________
DATE |
[ ] JUDGE [ ] MAGISTRATE |
[ ] SPECIAL JUSTICE [ ] CLERK |
|
|
|
|
|
FOR NOTARY PUBLIC’S USE ONLY: |
|
|
|
State of |
[ ] City [ ] County of |
|
Acknowledged, subscribed and sworn to before me this |
...................... day of |
, 20 |
by |
|
|
................................................................................ |
_____________________________________________________________ |
|
DATE |
NOTARY PUBLIC |
|
|
|
Notary Registration No |
(My commission expires |
) |
|
|
|
|
FORM DC-4001 (MASTER, PAGE TWO OF TWO) 07/13