
When using the online PDF tool by FormsPal, it is easy to fill out or edit Form Ddd 1404Aforpf here and now. Our tool is continually developing to deliver the best user experience achievable, and that is thanks to our dedication to continuous improvement and listening closely to comments from customers. Here's what you would have to do to begin:
Step 1: Click on the "Get Form" button above on this page to open our editor.
Step 2: With this advanced PDF tool, you'll be able to accomplish more than just fill out blanks. Try all of the features and make your forms look perfect with customized text added in, or adjust the original content to perfection - all backed up by an ability to add any pictures and sign it off.
With regards to the blank fields of this specific document, here is what you need to do:
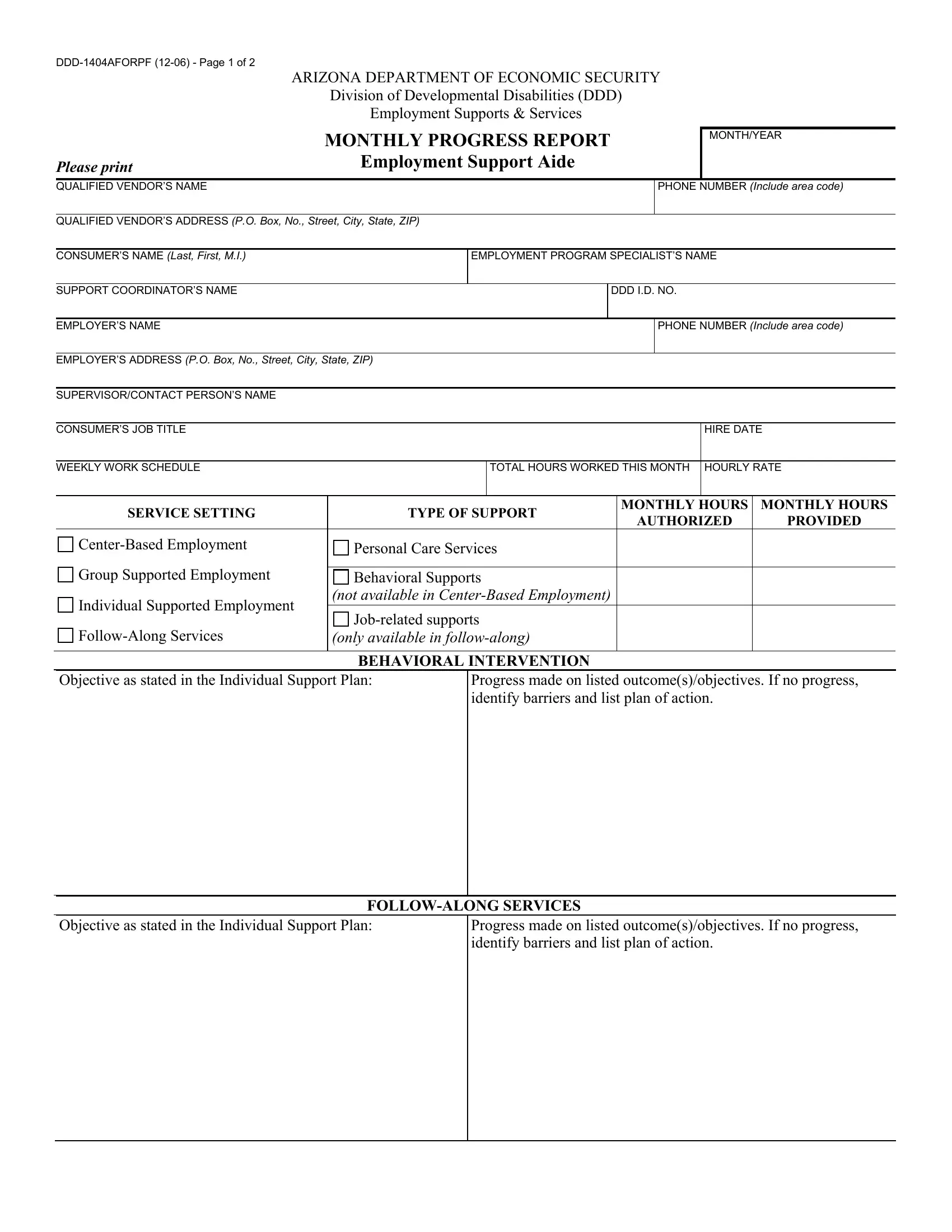
1. It's very important to fill out the Form Ddd 1404Aforpf accurately, thus be careful while filling in the segments that contain these blank fields:
2. After this array of fields is complete, it is time to add the needed particulars in Group Supported Employment, Individual Supported Employment, FollowAlong Services, Behavioral Supports, not available in CenterBased, Jobrelated supports, only available in followalong, BEHAVIORAL INTERVENTION, Objective as stated in the, Progress made on listed, Objective as stated in the, Progress made on listed, and FOLLOWALONG SERVICES so you're able to progress further.
3. This next section is mostly about Date, Service Hours, Summary of Services Rendered, Employment Support Aides, and Signature - fill in each one of these blanks.
A lot of people often make errors while filling out Signature in this section. Be sure you review what you type in here.
4. To move forward, this next part requires completing a handful of blank fields. Examples of these are QUALIFIED VENDOR, QUALIFIED VENDOR, QUALIFIED VENDOR, DATE, and Routing Original Support, which are vital to going forward with this particular process.
Step 3: Be certain that your information is accurate and click "Done" to progress further. Go for a free trial option with us and acquire direct access to Form Ddd 1404Aforpf - download or modify in your FormsPal account. FormsPal is focused on the confidentiality of all our users; we always make sure that all personal data coming through our editor is confidential.