
You could fill out ddd forms effortlessly with our online PDF tool. We are dedicated to providing you with the absolute best experience with our editor by constantly adding new capabilities and enhancements. Our tool has become even more user-friendly thanks to the latest updates! At this point, filling out documents is simpler and faster than ever before. Starting is simple! Everything you should do is stick to the next simple steps down below:
Step 1: Click the "Get Form" button above. It will open our tool so you can start filling out your form.
Step 2: Using our advanced PDF file editor, you can actually do more than just complete blank form fields. Express yourself and make your documents seem faultless with customized text incorporated, or optimize the original content to perfection - all supported by an ability to incorporate your personal photos and sign it off.
For you to finalize this form, make sure that you enter the necessary information in every blank:
1. While completing the ddd forms, ensure to include all important blanks in the relevant form section. It will help expedite the work, making it possible for your information to be processed fast and appropriately.
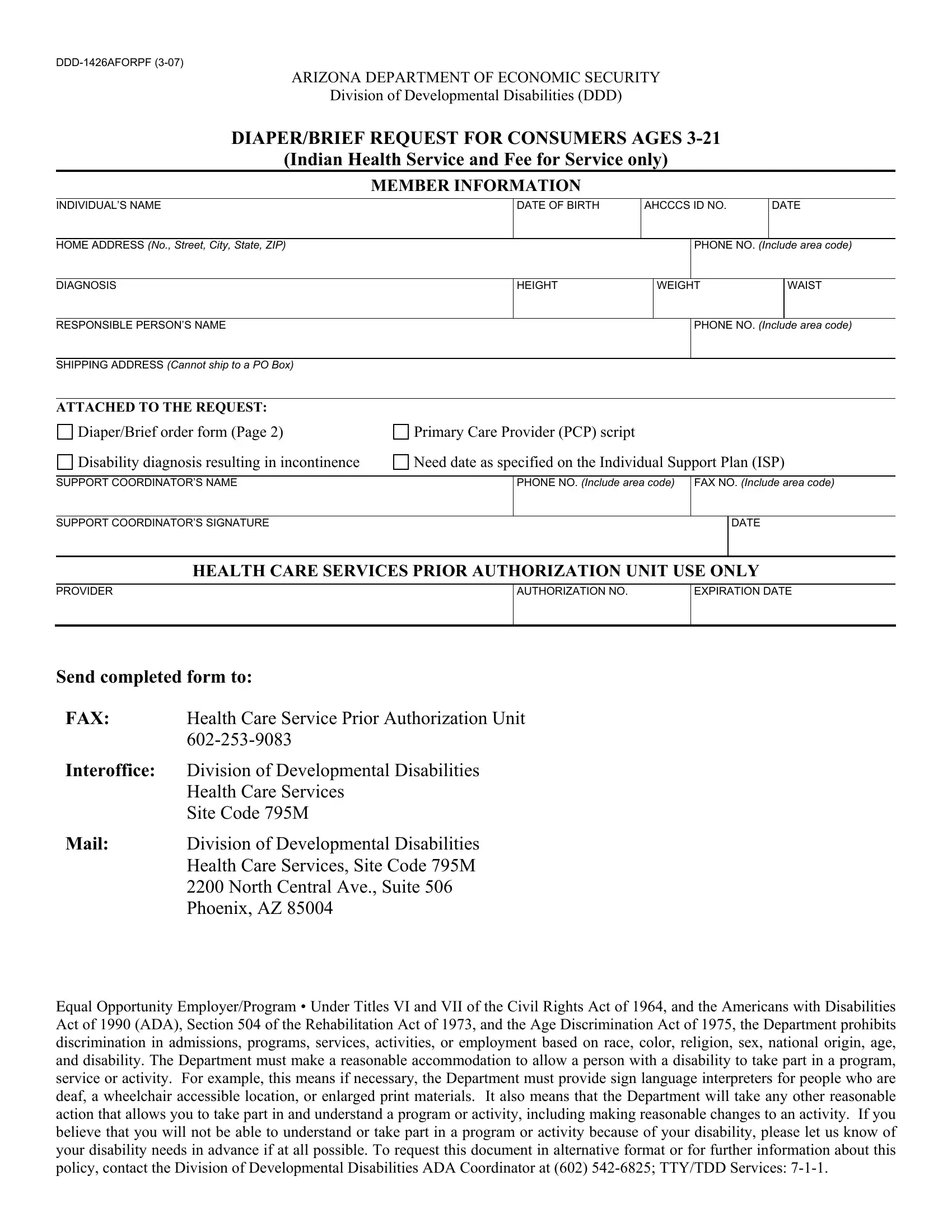
2. Given that the previous array of fields is complete, you have to insert the needed details in INDIVIDUALS NAME, Number of diapers used per day, DATE OF BIRTH, AHCCCS ID NO, DATE, Diaper Pamper Baby Dry lbs Cs, Diaper Pamper Baby Dry lbs Cs of, Diaper Pamper Baby Dry lbs Cs of, Diaper Pamper Baby Dry lbs Cs of, Diaper Pamper Baby Dry lbs Cs of, Diaper Pamper Baby Dry lbs Cs, Diaper Pamper Baby Dry lbs Cs, PullUp Goodnights SmallMedium, and PullUp Goodnights SmallMedium so you're able to go further.
A lot of people often make some errors while filling in PullUp Goodnights SmallMedium in this section. You should definitely review everything you type in right here.
3. Completing PullUp Goodnights SmallMedium, PullUp Goodnights LargeXLarge, PullUp Goodnights LargeXLarge, PullUp All Nights Medium lbs Cs, PullUp All Nights LargeXLarge, PullUp Protect Small inch waist, PullUp Protect Medium inch waist, PullUp Protect Large inch waist, Tab Type, Briefs Youth full fit inch waist, Briefs Small Stay Dry inch waist, Briefs Small Molicare inch waist, and Briefs Medium NuFit inch waist Cs is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!
4. Filling in Briefs Medium NuFit inch waist Cs, Briefs Medium Molicare inch waist, Briefs Large NuFit inch waist Cs, Briefs Large Molicare inch waist, and Briefs XLarge NuFit inch waist Cs is essential in the fourth stage - make sure to take your time and fill in each and every blank!
Step 3: Once you've glanced through the details provided, simply click "Done" to conclude your form. Join FormsPal today and easily gain access to ddd forms, prepared for downloading. All alterations made by you are kept , allowing you to customize the document later as needed. At FormsPal, we strive to make sure that your details are kept secure.