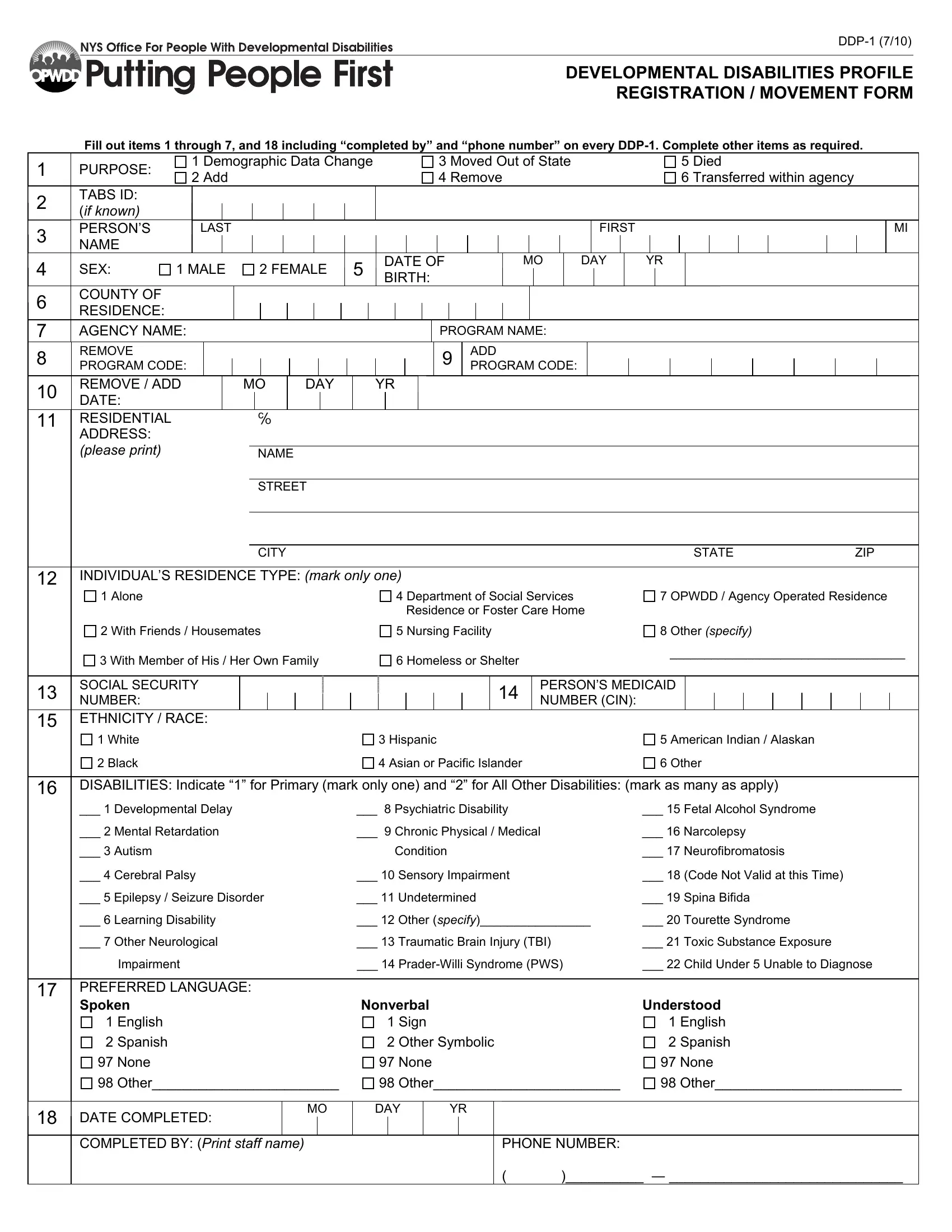
DDP-1 (7/10)
DEVELOPMENTAL DISABILITIES PROFILE
REGISTRATION / MOVEMENT FORM
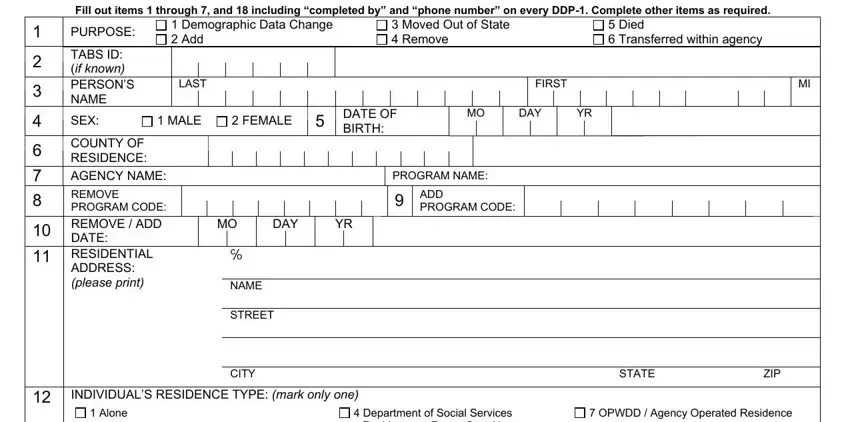
Fill out items 1 through 7, and 18 including “completed by” and “phone number” on every DDP-1. Complete other items as required.
|
1 |
PURPOSE: |
1 |
Demographic Data Change |
3 |
Moved Out of State |
5 Died |
|
2 |
Add |
4 |
Remove |
6 Transferred within agency |
|
|
|
2TABS ID: (if known)
3 |
PERSON’S |
LAST |
|
|
|
|
FIRST |
MI |
NAME |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4 |
SEX: |
1 MALE |
2 FEMALE |
5 |
DATE OF |
MO |
DAY |
YR |
BIRTH: |
|
|
|
|
|
|
|
|
|
6 |
COUNTY OF |
|
|
|
|
|
|
|
RESIDENCE: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
7 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
AGENCY NAME: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PROGRAM NAME: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
8 |
|
|
REMOVE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
9 |
ADD |
|
|
|
|
|
|
|
|
|
|
|
|
PROGRAM CODE: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PROGRAM CODE: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10 |
|
|
DATE:REMOVE / ADD |
|
|
MO |
|
DAY |
|
|
YR |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
11 |
|
|
RESIDENTIAL |
|
|
|
|
℅ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ADDRESS: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(please print) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
NAME |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
STREET |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CITY |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
STATE |
|
|
ZIP |
|
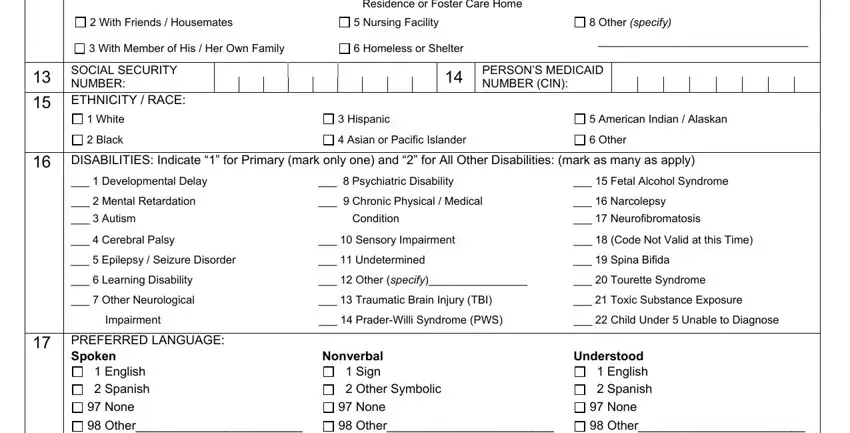
12INDIVIDUAL’S RESIDENCE TYPE: (mark only one)
|
1 |
Alone |
4 |
Department of Social Services |
7 |
OPWDD / Agency Operated Residence |
|
|
|
|
|
|
|
|
|
Residence or Foster Care Home |
|
|
|
|
|
|
|
|
|
|
|
2 |
With Friends / Housemates |
5 |
Nursing Facility |
|
8 |
Other (specify) |
|
3 With Member of His / Her Own Family |
6 |
Homeless or Shelter |
|
|
__________________________________ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
13 |
SOCIAL SECURITY |
|
|
|
|
|
|
|
|
|
14 |
PERSON’S MEDICAID |
|
|
|
|
|
|
|
|
NUMBER: |
|
|
|
|
|
|
|
|
|
NUMBER (CIN): |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
15ETHNICITY / RACE:
1 |
White |
3 |
Hispanic |
5 |
American Indian / Alaskan |
2 |
Black |
4 |
Asian or Pacific Islander |
6 |
Other |
16DISABILITIES: Indicate “1” for Primary (mark only one) and “2” for All Other Disabilities: (mark as many as apply)
___ 1 Developmental Delay |
___ |
8 Psychiatric Disability |
___ 15 Fetal Alcohol Syndrome |
___ 2 Mental Retardation |
___ |
9 Chronic Physical / Medical |
___ 16 Narcolepsy |
___ 3 Autism |
|
|
Condition |
___ 17 |
Neurofibromatosis |
___ 4 |
Cerebral Palsy |
___ 10 |
Sensory Impairment |
___ 18 (Code Not Valid at this Time) |
___ 5 Epilepsy / Seizure Disorder |
___ 11 Undetermined |
___ 19 |
Spina Bifida |
___ 6 |
Learning Disability |
___ 12 |
Other (specify)________________ |
___ 20 |
Tourette Syndrome |
___ 7 |
Other Neurological |
___ 13 |
Traumatic Brain Injury (TBI) |
___ 21 |
Toxic Substance Exposure |
|
Impairment |
___ 14 Prader-Willi Syndrome (PWS) |
___ 22 Child Under 5 Unable to Diagnose |
17PREFERRED LANGUAGE:
|
|
|
Spoken |
|
|
Nonverbal |
|
|
|
|
|
|
|
Understood |
1 |
English |
1 |
Sign |
|
|
|
|
|
|
|
1 |
English |
2 |
Spanish |
2 |
Other Symbolic |
|
2 |
Spanish |
|
|
|
97 None |
|
|
97 None |
|
|
|
|
|
|
|
97 None |
98 |
Other________________________ |
98 |
Other________________________ |
98 |
Other________________________ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MO |
|
|
DAY |
|
YR |
|
|
|
|
|
|
|
18 |
|
|
|
|
|
|
|
|
DATE COMPLETED: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
COMPLETED BY: (Print staff name) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PHONE NUMBER: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
( |
)__________ ― ______________________________ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
The DDP-1 is to be completed by all voluntary agency OPWDD-certified or funded programs or services.
Private schools may use either form DDP-1 or OMR 725.
GENERAL INSTRUCTIONS:
Items 1-7 and 18 should always be completed.
Complete items 8 and 10 if a person is leaving a program or 9 and 10 if a person is entering a program. Complete items 8, 9 and 10 if purpose #6, Transferred within agency, is marked.
Complete items 11-17 for anyone new to your agency, for anyone not previously registered in TABS, or if there is a question about whether a person has been previously registered in TABS.
1. Purpose:
1Select this response if information on a previous form should be updated or corrected.
2A person is added to a residence on the first day he/she sleeps in the residence. A person is added to a day program/service on the first day he/she receives services.
4If a person is leaving more than one program within the agency, each program must report the removal of that person from its rolls.
5The date of the person’s death should be entered in item 10, Remove/Add Date.
6Select this response if a person is changing programs (such as a residence) within the same agency. Complete items 8, 9 and 10 if this purpose is chosen.
2.TABS ID:
The minimum information required to register a person in TABS is the person’s name, sex, date of birth, and county of residence. This number may be up to 6 digits in length.
3. Name and 5. Date of Birth:
For each of these items, use the person’s birth certificate as the preferred source of the information. If not available, use the information as it appears on the person’s Medicaid card.
6. County of Residence:
This is the name of the county where the person resides. If adding this person to a residential program, use the name of the county where the residence is located.
8.& 9. Program Code (Remove & Add):
The Program code is an eight (8) digit number used to identify the program or service in TABS. Please contact the DDP Coordinator in your area if you are unsure of the correct code to use.
10. Remove/Add Date:
Enter the date of the event for choice 2-6 in item 1, Purpose. Enter a date if choice 1, Demographic Data Change, involves a change of address.
16. Disabilities:
Any disability indicated in this item should be officially documented in the person’s record including the signature of the diagnosing physician or psychologist.
17. Preferred Language:
Indicate which method of communication the person prefers to use.
18. Completed by:
This should contain the name and phone number (including area code) of the staff person who has completed this form. Please do not ask a parent, guardian or friend to complete the DDP-1.
If you have other questions about any item on the DDP-1, please consult the Users Guide.
Copies of the Guide may be obtained from your DDP Coordinator.