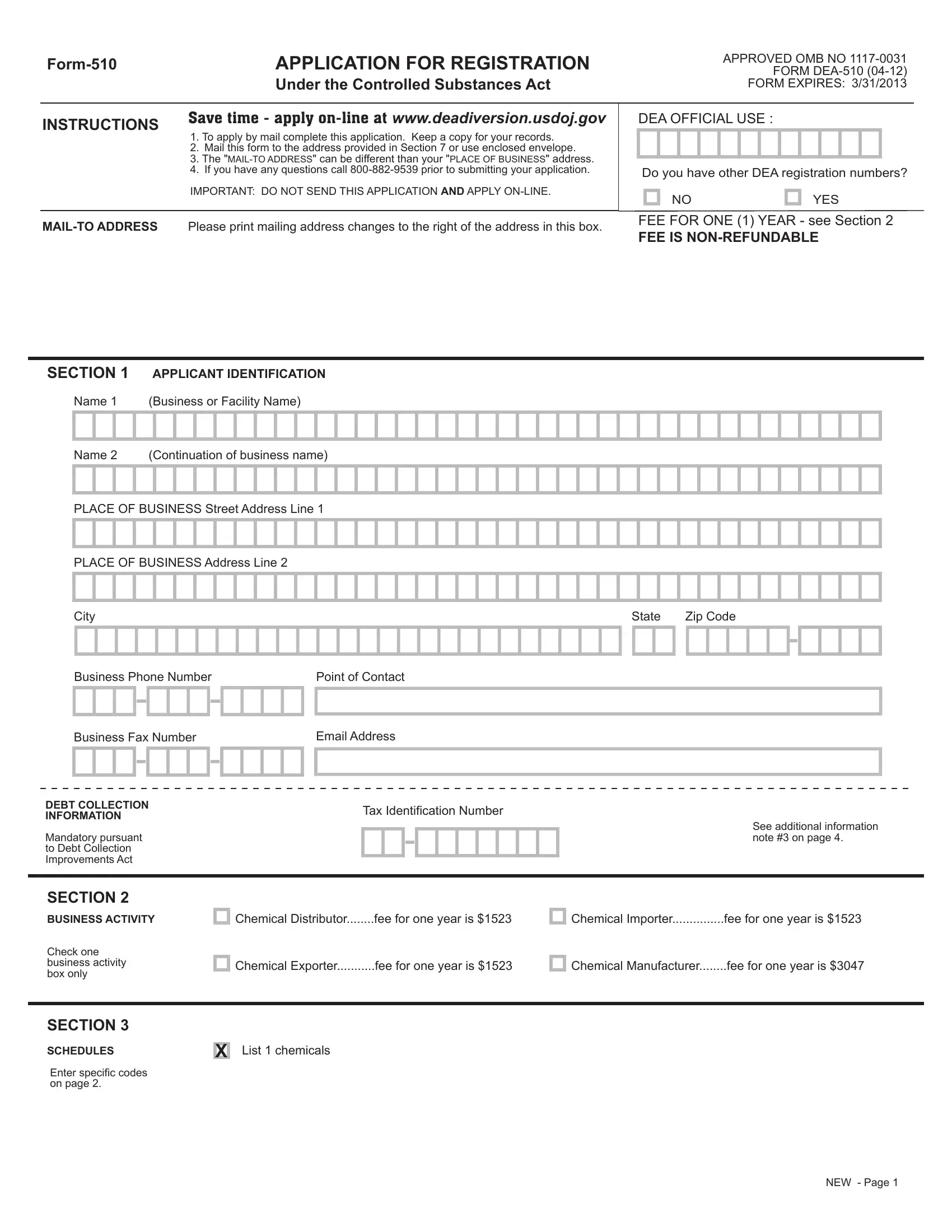
Navigating the complexities of regulatory compliance, the DEA Form 510 emerges as a critical instrument for entities embarking on activities governed under the Controlled Substances Act. Offering a streamlined pathway towards registration, this form encapsulates a detailed framework for applicants, ensuring adherence to federal mandates. From chemical distributors to importers, the Form 510 delineates specific categories of business activities, each associated with a unique fee structure, thereby simplifying the financial aspect of compliance. Moreover, the emphasis on liability questions within the form serves as a preemptive measure, meticulously screening applicants against a backdrop of legal constraints related to listed chemicals. A multifaceted document, the Form 510 also accommodates exemptions, notably for government officials or institutions, underscoring the DEA's commitment to facilitating a broad spectrum of legitimate chemical-related endeavors. Payment methodologies are meticulously outlined, providing applicants with a variety of options to fulfill their financial obligations, further testament to the form's user-centric design. Beyond its functional attributes, the Form 510 encapsulates a comprehensive approach to registration, marrying regulatory rigor with an accessible application process. Through an intricate balance of obligatory disclosures, fee structures, and operational specifics, the Form 510 stands as a cornerstone of regulatory compliance, guiding applicants through the DEA's stringent registration landscape.
| Question | Answer |
|---|---|
| Form Name | Form Dea 510 |
| Form Length | 4 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min |
| Other names | dea form 510, Isosafrole, Form-510, CSA |
APPLICATION FOR REGISTRATION |
|
|
Under the Controlled Substances Act |
APPROVED OMB NO
FORM EXPIRES: 3/31/2013
INSTRUCTIONS |
Save time - apply |
||
1. |
To apply by mail complete this application. Keep a copy for your records. |
||
|
|||
|
2. |
Mail this form to the address provided in Section 7 or use enclosed envelope. |
|
|
3. |
The |
|
|
4. |
If you have any questions call |
|
|
IMPORTANT: DO NOT SEND THIS APPLICATION AND APPLY |
||
|
|
||
Please print mailing address changes to the right of the address in this box. |
|||
DEA OFFICIAL USE :
Do you have other DEA registration numbers?
NO |
YES |
FEE FOR ONE (1) YEAR - see Section 2
FEE IS
SECTION 1 |
APPLICANT IDENTIFICATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||
|
Name 1 |
(Business or Facility Name) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Name 2 |
(Continuation of business name) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PLACE OF BUSINESS Street Address Line 1 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PLACE OF BUSINESS Address Line 2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
City |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
State |
Zip Code |
|
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Business Phone Number |
|
|
|
|
|
|
|
|
Point of Contact |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Business Fax Number |
|
|
|
|
|
|
|
|
Email Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DEBT COLLECTION |
|
|
|
|
|
|
|
|
|
|
|
Tax Identification Number |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||
INFORMATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
See additional information |
|
||||||||
Mandatory pursuant |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
note #3 on page 4. |
|
||||||||||||
to Debt Collection |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
Improvements Act |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
SECTION 2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
Chemical Distributor........fee for one year is $1523 |
|
|
|
Chemical Importer...............fee for one year is $1523 |
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||
BUSINESS ACTIVITY |
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Check one |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
business activity |
|
|
|
|
|
|
|
|
|
|
Chemical Exporter...........fee for one year is $1523 |
|
|
|
Chemical Manufacturer........fee for one year is $3047 |
|
|||||||||||||||||||||||||||||||||||||||||||||||
box only |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
SECTION 3
SCHEDULES
Enter specific codes on page 2.
X
List 1 chemicals
NEW - Page 1
SECTION 4
STATE LICENSE
NOT REQUIRED by this state
Enter your state license information if you are currently authorized to manufacture distribute, import, or export the listed chemicals for which you are applying under the laws of the state or jurisdiction in which you are operating or propose to operate.
State License Number
What state issued this license ? |
|
Expiration Date |
/ |
/ |
|
|
|
|
|
||
|
|
|
MM - DD - |
YYYY |
|
|
|
|
|
|
|
YES NO
SECTION 5
LIABILITY
IMPORTANT
All questions in this section must be answered.
1.Has the applicant ever been convicted of a crime in connection with listed chemical(s) under state or federal law, or is any such action pending?
Date(s) of incident
2.Has the applicant ever surrendered (for cause) or had a federal registration revoked, suspended, restricted, or denied, or is any such action pending?
Date(s) of incident
YES NO
YES NO
3. Has the applicant ever surrendered (for cause) or had a state professional license or registration revoked, suspended, denied, restricted, or placed on probation, or is any such action pending?
Date(s) of incident
YES NO
4. If the applicant is a corporation (other than a corporation whose stock is owned and traded by the public), association, partnership, or pharmacy, has any officer, partner, stockholder, or proprietor been convicted of a crime in connection with listed chemical(s) under state or federal law, or ever surrendered, for cause, or had a federal listed chemical/controlled registration revoked, suspended, restricted, denied, or ever had a state professional license or controlled substance substance registration revoked, suspended, denied, restricted or placed on probation, or is any such action pending?
Date(s) of incident
Note: If question 4 does not apply to you, be sure to mark 'NO'.
It will slow down processing of your application if you leave it blank.
EXPLANATION OF "YES" ANSWERS
Applicants who have answered "YES" to any of the four questions above must provide
a statement to explain each "YES" answer.
Use this space or attach a separate sheet and return with application
Liability question # |
|
Location(s) of incident: |
Nature of incident:
Disposition of incident:
SECTION 6 EXEMPTION FROM APPLICATION FEE
Check this box if the applicant is a federal, state, or local government official or institution. Does not apply to
Business or Facility Name of Fee Exempt Institution. Be sure to enter the address of this exempt institution in Section 1.
The undersigned hereby certifies that the applicant named hereon is a federal, state or local government official or institution, and is exempt from payment of the application fee.
FEE EXEMPT |
|
|
|
|
CERTIFIER |
|
|
|
|
|
Signature of certifying official (other than applicant) |
Date |
||
Provide the name and |
|
|
|
|
phone number of the |
|
|
|
|
Print or type name and title of certifying official |
Telephone No. (required for verification) |
|||
certifying official |
||||
SECTION 7
METHOD OF
PAYMENT
Check one form of payment only
Sign if paying by credit card
Make check payable to: Drug Enforcement Administration
Check See page 4 of instructions for important information.
American Express |
Discover |
|
Master Card |
Visa |
|||||||||||||||||||
Credit Card Number |
|
|
|
|
|
|
|
|
|
|
|
Expiration Date |
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Signature of Card Holder
Mail this form with payment to:
DEA Headquarters
ATTN: Registration Section/ODR
P.O. Box 2639
Springfield, VA
FEE IS
Printed Name of Card Holder
SECTION 8 |
I certify that the foregoing information furnished on this application is true and correct. |
|
|
|
APPLICANT'S |
|
|
|
|
SIGNATURE |
|
|
|
|
Signature of applicant (sign in ink) |
Date |
|||
|
||||
Sign in ink |
|
|
|
|
Print or type name and title of applicant
WARNING: 21 USC 843(d), states that any person who knowingly or intentionally furnishes false or fraudulent information in the application is subject to a term of imprisonment of not more than 4 years, and a fine under Title 18 of not more than $250,000, or both.
NEW - Page 3
C. SCHEDULE AND DRUG CODESzyxw Listed below are List 1 chemical codes. Check all chemical codes you handle, and mark if it is bulk or dosage form.
For more information, see our website at www.deadiversion.usdoj.gov, 21 CFR 1308, or call
If you bulk manufacture a chemical, check the "BULK?" column after the applicable class code.
If you manufacture the dosage form of a chemical, check the "DOSAGE?" column after the applicable code.
List 1
Chemical Name
Anthranilic Acid
Benzaldehyde
Benzyl Cyanide
Ephedrine
Ergonovine
Ergotamine
Ethylamine
Gamma Butyrolactone (GBL)
Hydriodic Acid
Hypophosphorous Acid and Salts
Iodine
Isosafrole
Methylamine
Nitroethane
Norpseudoephedrine
Phenylacetic Acid
Phenylpropanolamine
Piperidine
Piperonal
Propionic Anhydride
Pseudeophedrine
Red Phosphorous
Safrole
White Phosphorous
Code
8502
8530
8256
8735
8113
8675
8676
8678
2011
6695
6797
6699
8704
8520
8522
8115
8119
8332
6724
8317
8791
1225
2704
8750
8328
8112
6795
8323
6796
Bulk? Dosage?
WRITE IN ADDITIONAL CODES |
You may write in additional drug codes in this section. Attach a separate sheet if needed. |
NEW - Page 2
|
|
|
||
|
must enter a valid tax identification number (TIN). zyxwvutsrqpo |
|||
|
APPLICATION FOR REGISTRATION |
Supplementary Inst uctions and Information |
||
|
SECTION 1. APPLICANT IDENTIFICATION - Information must be ped or printed in the blocks provided to help red |
ce data en ry errors. A physical address is required in |
||
|
address line 1; a post office box or continuation of address may be entered in address line 2. Fee exempt applicant m |
st list the addre of the fee exempt institution. A licant |
||
Debt collection information is mandatory pursuant to the Debt Collection Improvement Act of 1996.
SECTION 2. BUSINESS ACTIVITY - Indicate only one. Indicate only one business activity on this application. Each type of business activity requires a separate application. If you are registered with DEA to manufacture, import, export, or distribute/dispense controlled substances, you do not have to register for the same activities with drug products that contain List 1 chemicals.
クYou are required to register as a "manufacturer" if you manufacture a List 1 chemical and then distribute it. You do not have to register if you manufacture a List 1 chemical for internal consumption with no subsequent distribution of it.
クRegistration as an importer conveys distribution privileges only for those List 1 chemicals imported.
SECTION 3. DRUG SCHEDULES - Applicants is registering for l List 1 chemicals on this application. However, applicants must still comply with state requirements; federal registration does not overrule state restrictions.
3B. MANUFACTURER ONLY - Mark the appropriate box to indicate if you are manufacturing List 1 chemicals in bulk or dosage form.
3C. CHEMICAL CODES - Applicant must check all List 1 chemicals to be handled and indicate if the chemical is in bulk or dosage form.
SECTION 4. STATE LICENSE(S) - Federal registration by DEA is based upon the applicant's compliance with applicable state and local laws. Applicant should contact the local state licensing authority prior to completing this application. If your state requires a license, provide that information and attach a copy to this application. If YOUR STATE DOES NOT REQUIRE A LICENSE, MARK AN "X" IN THE BOX TO INDICATE IT NOT REQUIRED BY YOUR STATE.
SECTION 5. LIABILITY - Applicant must answer all four questions for the application to be accepted for processing. If you answer "Yes" to a question, provide an explanation in the space provided. If you answer "Yes" to several of the questions, then you must provide a separate explanation describing the date, location, nature, and result of each incident. If additional space is required, you may attach a separate page.
SECTION 6. EXEMPTION FROM APPLICATION FEE - Exemption from payment of application fee is limited to federal, state or local government official or institution. The applicant's superior or agency officer must certify exempt status. The signature, authority title, and telephone number of the certifying official (other than the applicant) must be provided. The address of the fee exempt institution must appear in Section 1.
SECTION 7. METHOD OF PAYMENT - Indicate the desired method of payment. Make checks payable to "Drug Enforcement Administration".
SECTION 8. APPLICANT'S SIGNATURE - Applicant MUST sign in this section or application will be returned. Card holder signature in section 7 does not fulfill this requirement.
NOTICE TO REGISTRANTS MAKING PAYMENT BY CHECK
Authorization to Convert Your Check: If you send us a check to make your payment, your check will be converted into an electronic fund transfer. "Electronic fund transfer" is the term used to refer to the process in which we electronically instruct your financial institution to transfer funds from your account to our account, rather than processing your check. By sending your completed, signed check to us, you authorize us to copy your check and to use the account information from your check to make an electronic fund transfer from your account for the same amount as the check. If the electronic fund transfer cannot be processed for technical reasons, you authorize us to process the copy of your check.
Insufficient Funds: The electronic funds transfer from your account will usually occur within 24 hours, which is faster than a check is normally processed. Therefore, make sure there are sufficient funds available in your checking account when you send us your check. If the electronic funds transfer cannot be completed because of insufficient funds, we may try to make the transfer up to two more times.
Transaction Information: The electronic fund transfer from your account will be on the account statement you receive from your financial institution. However, the transfer may be in a different place on your statement than the place where your checks normally appear. For example, it may appear under "other withdrawals" or "other transactions". You will not receive your original check back from your financial institution. For security reasons, we will destroy your original check, but we will keep a copy of the check for
Your Rights: You should contact your financial institution immediately if you believe that the electronic fund transfer reported on your account statement was not properly authorized or is otherwise incorrect. Consumers have protections under Federal law called the Electronic Fund Transfer Act for an unauthorized or incorrect electronic fund transfer.
ADDITIONAL INFORMATION
No registration will be issued unless a completed application form has been received (21 CFR 1301.13).
In accordance with the Paperwork Reduction Act of 1995, no person is required to respond to a collection of information unless it displays a valid OMB control number. The OMB number for this collection is
The Debt Collection Improvements Act of 1996 (31 U.S.C. §7701) requires that you furnish your Taxpayer Identification Number (TIN) or Social Security Number (SSN) on this application. This number is required for debt collection procedures if your fee is not collectible.
PRIVACY ACT NOTICE: Providing information other than your SSN or TIN is voluntary; however, failure to furnish it will preclude processing of the application. The authorities for collection of this information are §§302 and 303 of the Controlled Substances Act (CSA) (21 U.S.C. §§822 and 823). The principle purpose for which the information will be used is to register applicants pursuant to the CSA. The information may be disclosed to other Federal law enforcement and regulatory agencies for law enforcement and regulatory purposes, State and local law enforcement and regulatory agencies for law enforcement and regulatory purposes, and person registered under the CSA for the purpose of verifying registration. For further guidance regarding how your information may be used or disclosed, and a complete list of the routine uses of this collection, please see the DEA System of Records Notice "Controlled Substances Act Registration Records"
Your Local |
CONTACT INFORMATION |
DEA Office |
All offices are listed on website |
|
(800, 877, and 888 are |
INTERNET:
Information can be found on our website at www.deadiversion.usdoj.gov TELEPHONE: Headquarters Call Center: (800)
WRITTEN INQUIRIES:
Drug Enforcement Administration
Registration Section/ODR
P.O. Box 2639
Springfield, VA
NEW INST - Page 4