DH use only: Check No. _______ Check Amount _______________
Date Received _______________ Receipt No. ___________________
Permit No. ___________________ Date Issued ___________________
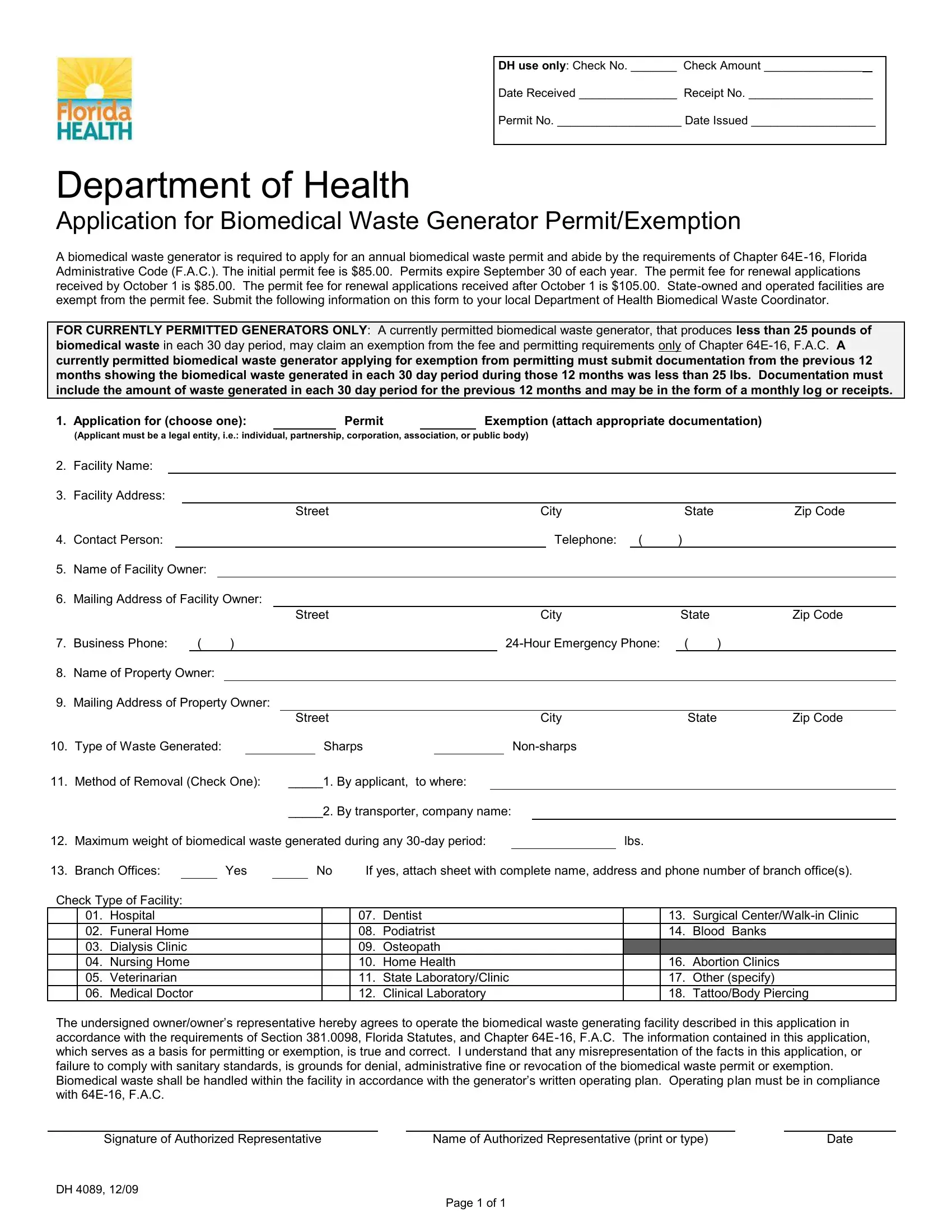
Department of Health
Application for Biomedical Waste Generator Permit/Exemption
A biomedical waste generator is required to apply for an annual biomedical waste permit and abide by the requirements of Chapter 64E-16, Florida Administrative Code (F.A.C.). The initial permit fee is $85.00. Permits expire September 30 of each year. The permit fee for renewal applications received by October 1 is $85.00. The permit fee for renewal applications received after October 1 is $105.00. State-owned and operated facilities are exempt from the permit fee. Submit the following information on this form to your local Department of Health Biomedical Waste Coordinator.
FOR CURRENTLY PERMITTED GENERATORS ONLY: A currently permitted biomedical waste generator, that produces less than 25 pounds of biomedical waste in each 30 day period, may claim an exemption from the fee and permitting requirements only of Chapter 64E-16, F.A.C. A
currently permitted biomedical waste generator applying for exemption from permitting must submit documentation from the previous 12 months showing the biomedical waste generated in each 30 day period during those 12 months was less than 25 lbs. Documentation must include the amount of waste generated in each 30 day period for the previous 12 months and may be in the form of a monthly log or receipts.
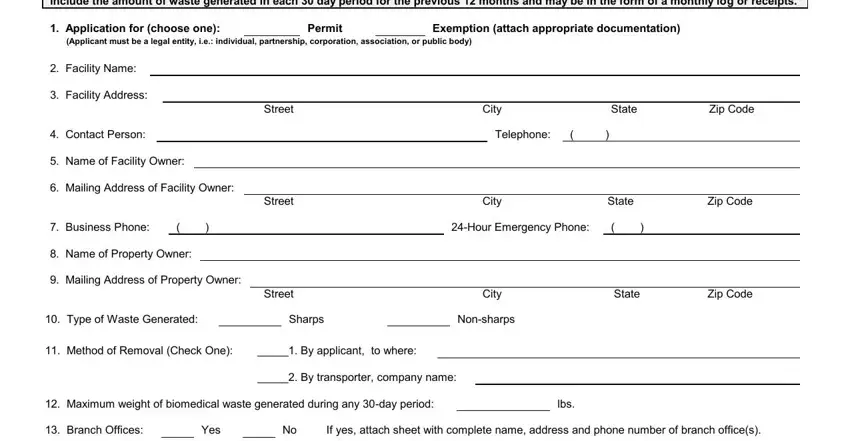
1. Application for (choose one): |
|
Permit |
|
Exemption (attach appropriate documentation) |
(Applicant must be a legal entity, i.e.: individual, partnership, corporation, association, or public body)
2.Facility Name:
3.Facility Address:
|
Street |
City |
|
State |
Zip Code |
4. Contact Person: |
|
|
Telephone: |
( |
) |
|
5.Name of Facility Owner:
6.Mailing Address of Facility Owner:
|
|
Street |
City |
State |
Zip Code |
7. Business Phone: |
( |
) |
24-Hour Emergency Phone: |
( |
) |
8.Name of Property Owner:
9.Mailing Address of Property Owner:
|
|
|
|
|
|
Street |
|
|
|
|
|
|
City |
State |
Zip Code |
10. |
Type of Waste Generated: |
|
|
|
|
Sharps |
|
|
|
|
Non-sharps |
|
|
11. |
Method of Removal (Check One): |
_____1. |
By applicant, |
to where: |
|
|
|
|
|
|
|
|
|
_____2. |
By transporter, company name: |
|
|
|
12. |
Maximum weight of biomedical waste generated during any 30-day period: |
|
lbs. |
|
13. |
Branch Offices: |
|
|
Yes |
|
|
No |
If yes, attach sheet with complete name, address and phone number of branch office(s). |
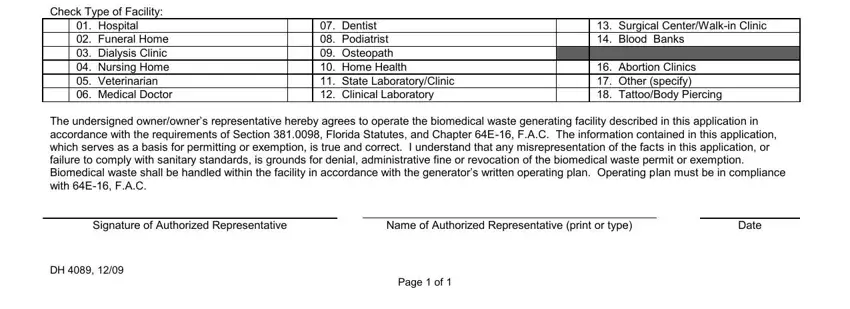
Check Type of Facility:
|
01. |
Hospital |
|
07. |
Dentist |
|
13. |
Surgical Center/Walk-in Clinic |
|
02. |
Funeral Home |
|
08. |
Podiatrist |
|
14. |
Blood Banks |
|
03. |
Dialysis Clinic |
|
09. |
Osteopath |
|
|
|
|
04. |
Nursing Home |
|
10. |
Home Health |
|
16. |
Abortion Clinics |
|
05. |
Veterinarian |
|
11. |
State Laboratory/Clinic |
|
17. |
Other (specify) |
|
06. |
Medical Doctor |
|
12. |
Clinical Laboratory |
|
18. |
Tattoo/Body Piercing |
The undersigned owner/owner’s representative hereby agrees to operate the biomedical waste generating facility described in this application in accordance with the requirements of Section 381.0098, Florida Statutes, and Chapter 64E-16, F.A.C. The information contained in this application, which serves as a basis for permitting or exemption, is true and correct. I understand that any misrepresentation of the facts in this application, or
failure to comply with sanitary standards, is grounds for denial, administrative fine or revocation of the biomedical waste permit or exemption. Biomedical waste shall be handled within the facility in accordance with the generator’s written operating plan. Operating plan must be in compliance
with 64E-16, F.A.C.
Signature of Authorized Representative |
Name of Authorized Representative (print or type) |
Date |
DH 4089, 12/09
Page 1 of 1