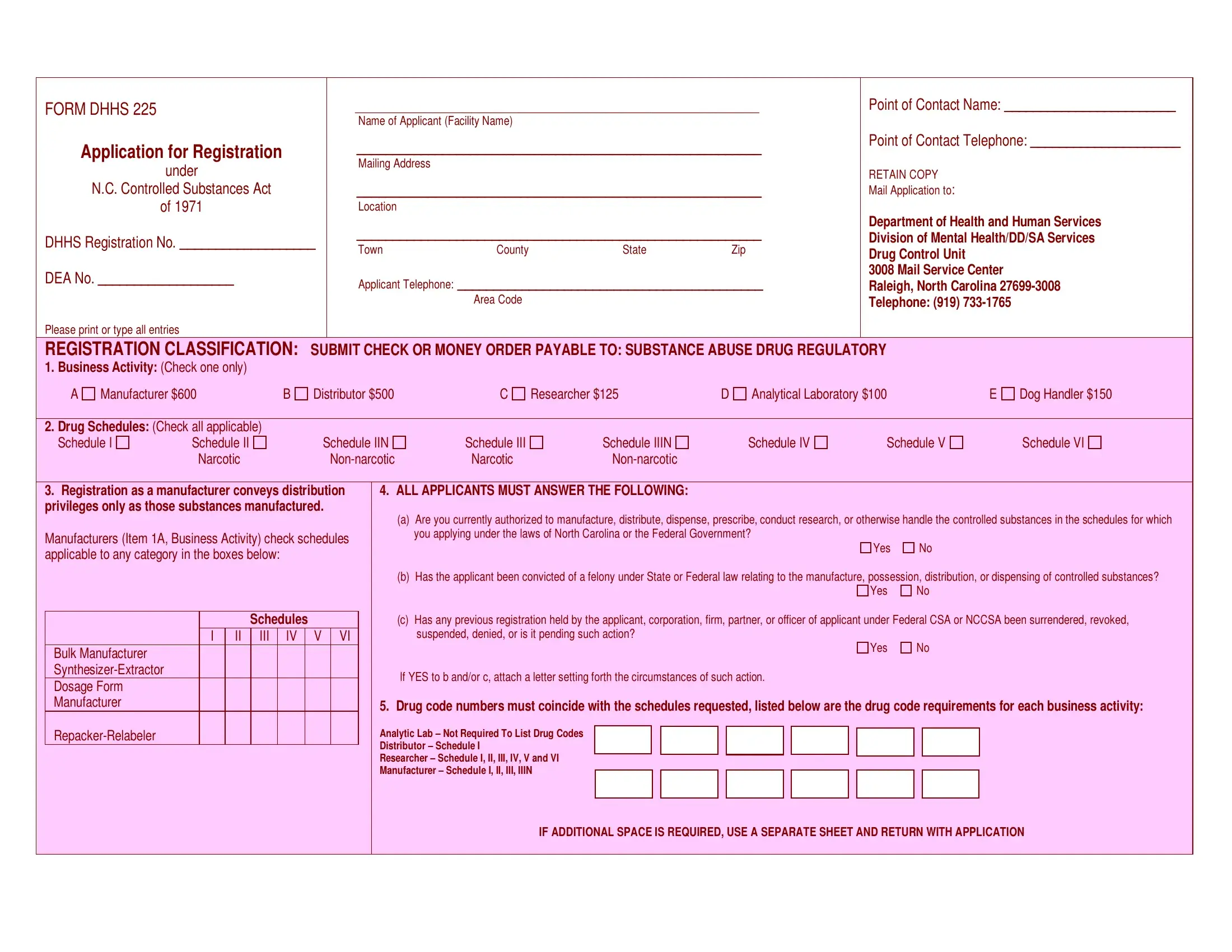
Getting to know the DHHS 225 form is essential for facilities and individuals that handle controlled substances under the N.C. Controlled Substances Act of 1971. This comprehensive form is a pivotal tool used in the application process for registering with the Department of Health and Human Services. With sections dedicated to basic identification details such as the name of the applicant or facility and point of contact information, it serves as the initial step towards compliance with state regulations. Applicants are required to select their business activity, ranging from manufacturers and distributors to researchers and dog handlers, with corresponding fees based on the category. It also necessitates the identification of the controlled substance schedules the applicant intends to work with, underscoring the strict oversight on narcotic and non-narcotic substances. Furthermore, the form prompts applicants to disclose any past felony convictions related to controlled substances or any previous registration issues, ensuring only qualified entities handle these potent materials. Completing the DHHS 225 requires thoroughness, as it involves not just basic facility information but detailed compliance aspects further ensuring the safe and legal handling of controlled substances within North Carolina.
| Question | Answer |
|---|---|
| Form Name | Form Dhhs 225 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | dhhs form 226 and 227, dhhs form 226 d, form dhhs 225 c, dhhs 226 |
|
FORM DHHS 225 |
|
|
|
|
|
|
|
|
|
|
|
|
____________________________________________________ |
|
|
|
|
Point of Contact Name: ________________________ |
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Name of Applicant (Facility Name) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
Application for Registration |
|
|
|
|
|
_________________________________________________________ |
|
|
|
|
Point of Contact Telephone: _____________________ |
|
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||
|
|
|
|
under |
|
|
|
|
|
|
Mailing Address |
|
|
|
|
|
|
|
|
|
|
|
RETAIN COPY |
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
N.C. Controlled Substances Act |
|
|
|
|
|
_________________________________________________________ |
|
|
|
|
Mail Application to: |
|
|
|||||||||||||||||||||
|
|
|
|
of 1971 |
|
|
|
|
|
|
Location |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
_________________________________________________________ |
|
|
|
|
Department of Health and Human Services |
|
|||||||||||||||
|
DHHS Registration No. ___________________ |
|
|
|
|
|
Division of Mental Health/DD/SA Services |
|
|||||||||||||||||||||||||||||
|
|
Town |
County |
|
State |
|
|
Zip |
|
||||||||||||||||||||||||||||
|
|
|
|
|
Drug Control Unit |
|
|
||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
DEA No. ___________________ |
|
|
|
|
|
|
Applicant Telephone: ___________________________________________ |
3008 Mail Service Center |
|
|
||||||||||||||||||||||||||
|
|
|
|
|
|
|
Raleigh, North Carolina |
|
|||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Area Code |
|
|
|
|
|
|
|
|
|
|
|
Telephone: (919) |
|
|
|||
|
Please print or type all entries |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
REGISTRATION CLASSIFICATION: SUBMIT CHECK OR MONEY ORDER PAYABLE TO: SUBSTANCE ABUSE DRUG REGULATORY |
|
|
|
|
|
|||||||||||||||||||||||||||||||
|
1. Business Activity: (Check one only) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
A |
Manufacturer $600 |
B |
Distributor $500 |
C |
Researcher $125 |
D |
Analytical Laboratory $100 |
|
|
E |
Dog Handler $150 |
|
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2. Drug Schedules: (Check all applicable) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
Schedule I |
|
Schedule II |
|
|
|
Schedule IIN |
Schedule III |
|
Schedule IIIN |
|
|
Schedule IV |
Schedule V |
Schedule VI |
|
||||||||||||||||||||
|
|
|
|
|
Narcotic |
|
|
|
|
Narcotic |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
3. Registration as a manufacturer conveys distribution |
|
|
|
4. ALL APPLICANTS MUST ANSWER THE FOLLOWING: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
|
privileges only as those substances manufactured. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(a) |
Are you currently authorized to manufacture, distribute, dispense, prescribe, conduct research, or otherwise handle the controlled substances in the schedules for which |
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
|
Manufacturers (Item 1A, Business Activity) check schedules |
|
|
|
|
you applying under the laws of North Carolina or the Federal Government? |
|
|
|
|
|
|
|||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Yes |
No |
|
|
|||||||||||||||||
|
applicable to any category in the boxes below: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
(b) |
Has the applicant been convicted of a felony under State or Federal law relating to the manufacture, possession, distribution, or dispensing of controlled substances? |
|
||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Yes |
No |
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Schedules |
|
|
|
|
|
(c) |
Has any previous registration held by the applicant, corporation, firm, partner, or officer of applicant under Federal CSA or NCCSA been surrendered, revoked, |
|
|||||||||||||||||||||
|
|
|
|
|
|
I |
|
II |
III |
|
|
IV |
|
V |
VI |
|
|
|
|
suspended, denied, or is it pending such action? |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
Bulk Manufacturer |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Yes |
No |
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
If YES to b and/or c, attach a letter setting forth the circumstances of such action. |
|
|
|
|
|
|
|||||||||||||||
|
|
Dosage Form |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
Manufacturer |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
5. Drug code numbers must coincide with the schedules requested, listed below are the drug code requirements for each business activity: |
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Analytic Lab – Not Required To List Drug Codes |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Distributor – Schedule I |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Researcher – Schedule I, II, III, IV, V and VI |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Manufacturer – Schedule I, II, III, IIIN |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
IF ADDITIONAL SPACE IS REQUIRED, USE A SEPARATE SHEET AND RETURN WITH APPLICATION |
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|

AUTHORIZED INDIVIDUAL |
|
|
|
|
|
|
|
__________________ |
________________________________ |
_________________________________ |
______________________________ |
Date |
Print or Type Name |
Signature |
Official Title |