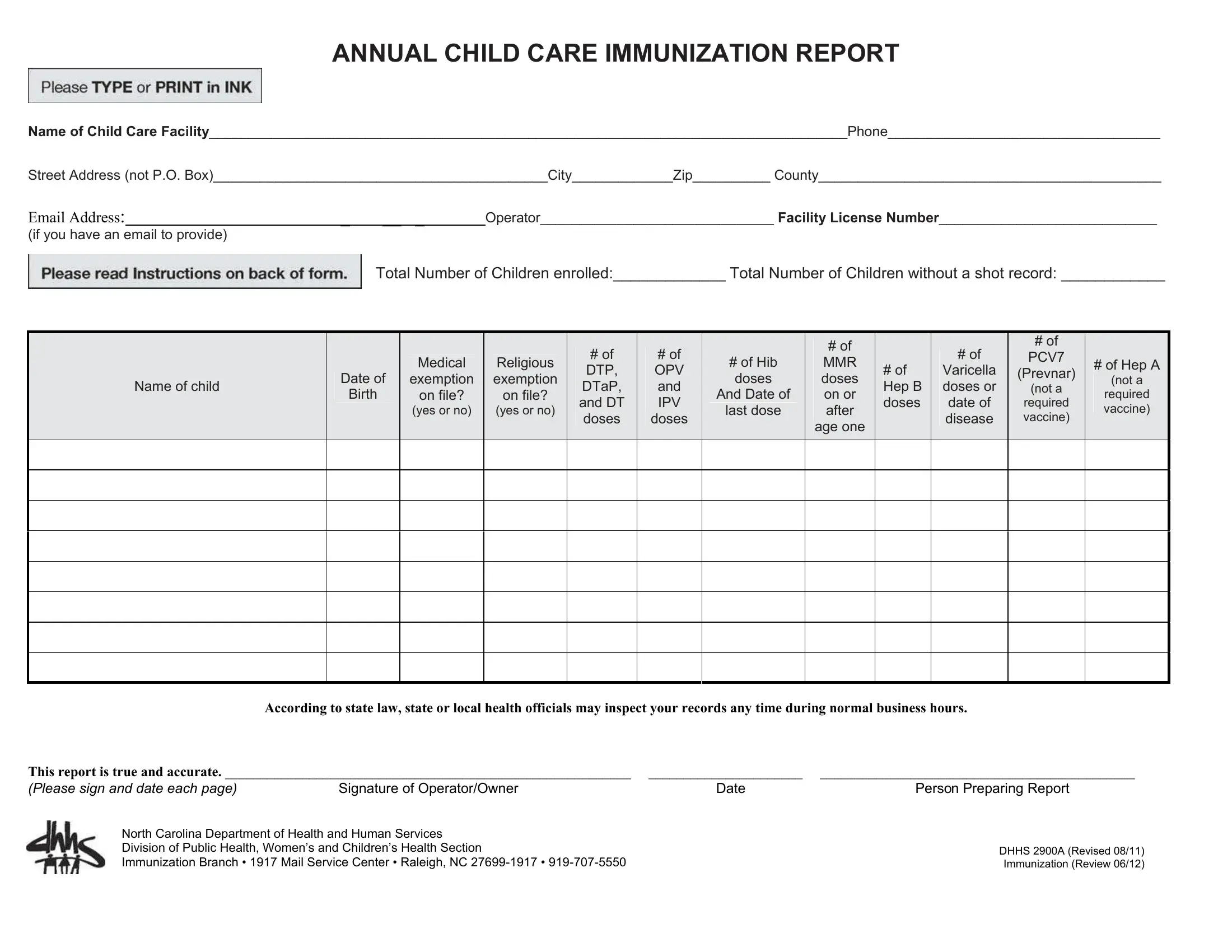
The DHHS 2900A form plays a crucial role for child care facilities in North Carolina, serving as the annual immunization report that operators must submit to fulfill legal requirements ensuring all enrolled children are adequately immunized. Detailing the name of the child care facility, contact information, and the total enrollment figures, it also meticulously records individual immunization statuses of the children, including exemptions for medical or religious reasons. The form comprehensively lists the required vaccines, such as DTP, DTaP, IPV, Hib, MMR, Varicella, and Hep B, alongside recommended ones like PCV7 (Prevnar) and Hep A, making it easier for facilities to track and report vaccination coverage. Necessary for yearly statistical analysis and in alignment with North Carolina Law (G.S. 130A-155), it underscores a child care operator's duty to maintain high immunization standards, allowing health officials to inspect records during business hours. The provision to use alternative tracking systems if they meet state criteria offers flexibility, while the mandate to have medical exemptions documented by a licensed doctor and religious exemptions by a parent statement confirms the thoroughness required in safeguarding children's health against preventable diseases. This form not only represents a straightforward compliance document but a critical public health tool in monitoring immunization rates within child care settings.
| Question | Answer |
|---|---|
| Form Name | Form Dhhs 2900A |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | dhhs 2900a, Hib, PCV7, DHHS |
ANNUAL CHILD CARE IMMUNIZATION REPORT
Name of Child Care Facility__________________________________________________________________________________Phone___________________________________
Street Address (not P.O. Box)___________________________________________City_____________Zip__________ County____________________________________________
EMAIL ADDRESS:_ __ _ Operator______________________________ Facility License Number____________________________
(if you have an email to provide)
Total Number of Children enrolled:_____________ Total Number of Children without a shot record: ____________
Name of child
Date of
Birth
Medical
exemption
on file?
(yes or no)
Religious
exemption
on file?
(yes or no)
# of |
# of |
DTP, |
OPV |
DTaP, |
and |
and DT |
IPV |
doses |
doses |
|
|
|
|
#of Hib doses
And Date of
last dose
#of
MMR
doses
on or
after
age one
|
|
|
|
# of |
|
# of |
|
# of |
PCV7 |
|
|
Varicella |
(Prevnar) |
|
|
Hep B |
|
doses or |
(not a |
|
doses |
|
date of |
required |
|
|
|
disease |
vaccine) |
|
|
|
|
|
|
|
|
|
|
# of Hep A
(not a
required vaccine)
According to state law, state or local health officials may inspect your records any time during normal business hours.
This report is true and accurate. __________________________________________________________ ______________________ _____________________________________________
(Please sign and date each page) |
Signature of Operator/Owner |
Date |
Person Preparing Report |
North Carolina Department of Health and Human Services |
|
|
|
Division of Public Health, Women’s and Children’s Health Section |
|
DHHS 2900A (Revised 08/11) |
|
|
|
|
|
Immunization Branch • 1917 Mail Service Center • Raleigh, NC |
|
Immunization (Review 06/12) |
|
Purpose: To provide child care operators with a means of fulfilling their legal obligations to assure that all children are properly immunized. This form is required by North Carolina Law (G.S.
Instructions: (Review the enclosed handout “Children in Child Care – What SHOTS Do They Need”? before completing this report.)
Note: If you have a system for tracking immunizations at your center and can provide a computer printout that includes the same information as listed on this form, you can submit that printout instead of completing this form. The printout must be signed by the Operator. The printout must be mailed to the Immunization Branch and your local health department.
Complete and mail this report by December 1. Press firmly to assure that all copies are readable. Complete the top portion of this form by filling in your facility information. Include facility license number. If your center is closed, please write closed across the form and mail it to the Immunization Branch
If your center has no children enrolled, please write zero in the total enrollment line and mail in the form.
For each child in your facility, enter their first name, their last name and their date of birth. Initials are not acceptable. You do not need to include school aged children who are enrolled in school.
For children with medical or religious exemptions on file enter ‘YES’ in the appropriate column.
Medical Exemption: A doctor licensed to practice medicine in NC must sign, date, and put in writing that a specific immunization is or may be harmful to a child’s health for a specific reason. Medical exemption statements are required by law to be on file at the facility and should state how long the exemption will last.
Religious Exemption: Parents who claim a religious objection to immunizations must provide to the facility a signed, dated statement indicating that receiving immunizations is against their bona fide religious beliefs. Religious Exemption Statements are required by law to be on file at the facility.
Enter the total number of doses of each vaccine the child has received.
The last two vaccines listed in the chart (PCV7 or Prevnar and Hep A) are recommended vaccines and not required vaccines for children in child care to have. If the child has received doses of these vaccines, please put the number of doses in the appropriate box, if they have not received any Prevnar or Hep A, you can put a zero or leave blank.
The operator and the person completing the report must sign and date it. Unsigned reports will be returned for signature. As soon as you have completed this report:
Immunization Branch
NC Department of Health and Human Services Division of Public Health
1917 Mail Service Center
Raleigh, NC
Mail the yellow copy to: Your Local Health Department Immunization Program
Keep the pink copy for your records.