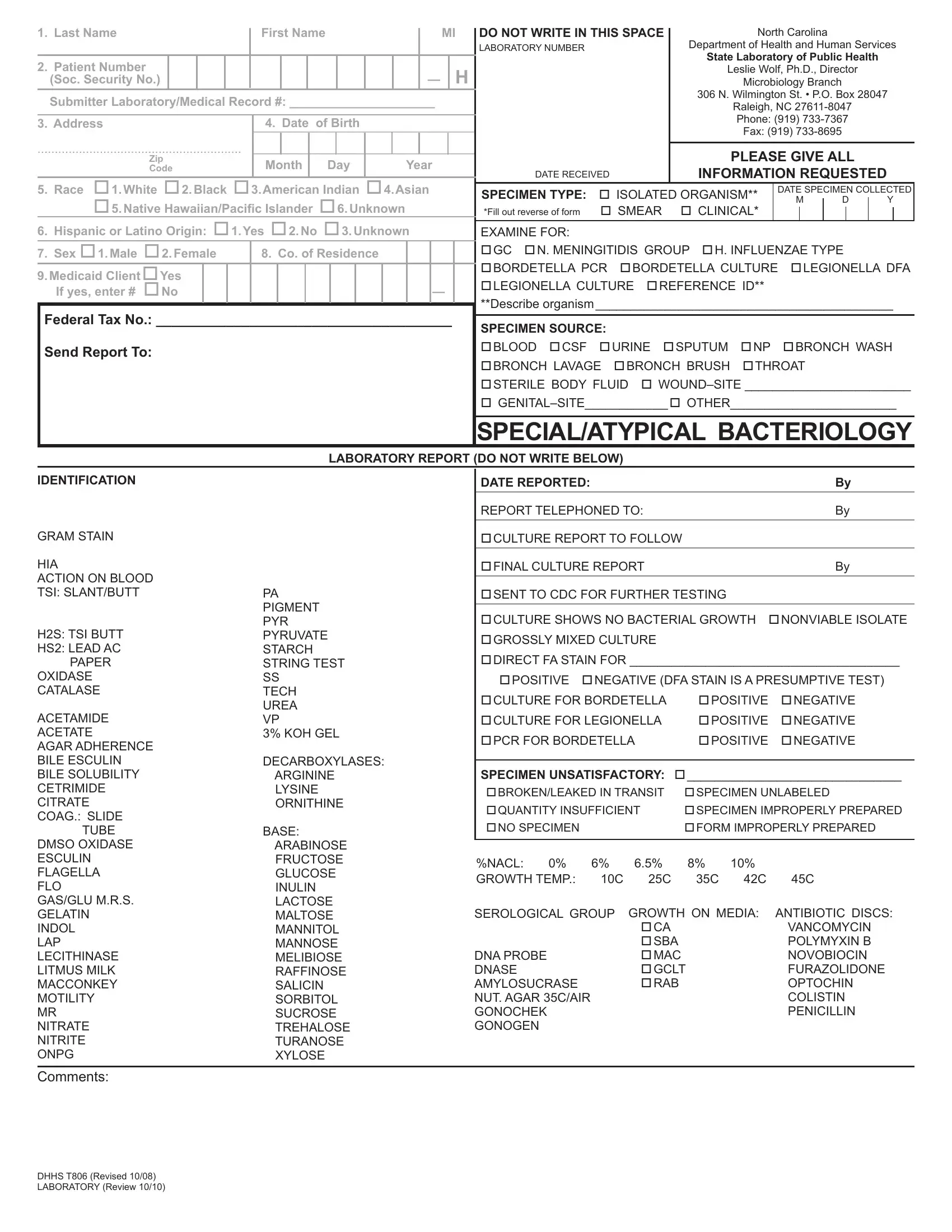
Understanding the complexities and requirements of medical documentation is crucial for ensuring accurate and timely patient care, especially within the public health sector. The DHHS T806 form, a vital document issued by the North Carolina Department of Health and Human Services and its State Laboratory of Public Health, serves a significant role in this process. Primarily used for submitting specimens for laboratory analysis, this form captures detailed patient information, which includes but is not limited to personal data, specimen type, collection dates, and tests required. Designed to streamline the identification, isolation, and confirmation of human disease-producing microorganisms, the form requires precise completion to avoid any delay or compromise in the diagnostic process. It uniquely combines epidemiological data collection with clinical specimen details, thereby aiding in public health monitoring and response. The form not only facilitates the laboratory's operational efficiency but also ensures that patients are accurately diagnosed and treated, based on the results of the tests conducted. As such, the DHHS T806 form embodies the intersection of patient care, laboratory science, and public health surveillance, highlighting its importance in safeguarding community health.
| Question | Answer |
|---|---|
| Form Name | Form Dhhs T806 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | dhhs t806 nc slph t806 form |
1. Last Name |
First Name |
|
|
|
MI |
|
DO NOT WRITE IN THIS SPACE |
|
North Carolina |
|
|
|
|
|
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
LABORATORY NUMBER |
|
Department of Health and Human Services |
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
State Laboratory of Public Health |
|
|
|||||||||
2. Patient Number |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
H |
|
|
|
Leslie Wolf, Ph.D., Director |
|
|
||||||||||||
(Soc. Security No.) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
— |
|
|
|
|
|
|
Microbiology Branch |
|
|
|
|
|
|||||||||
Submitter Laboratory/Medical Record #: _____________________ |
|
|
|
|
|
|
|
306 N. Wilmington St. • P.O. Box 28047 |
|||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
Raleigh, NC |
|
|
|||||||||||||||||||||||||||
3. Address |
4. Date |
of Birth |
|
|
|
|
|
|
|
|
|
|
|
Phone: (919) |
|
|
|||||||||||||||||||||
|
|
|
|
|
|
________________________________ |
|
|
|
|
Fax: (919) |
|
|
|
|
|
|||||||||||||||||||||
........................................................... |
|
|
|
________________________________ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
PLEASE GIVE ALL |
|
|
|||||||||||||||||||||||||||
|
Zip |
Month |
|
Day |
Year |
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
|
Code |
|
|
|
|
|
|
DATE RECEIVED |
INFORMATION REQUESTED |
|
|
||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
5. Race |
1.White 2.Black 3.American Indian 4.Asian |
|
|
|
|||||||||||||||||||||||||||||||||
|
SPECIMEN TYPE: |
ISOLATED ORGANISM** |
DATE SPECIMEN COLLECTED |
||||||||||||||||||||||||||||||||||
|
5. Native Hawaiian/Paciic Islander 6.Unknown |
|
|
|
|
|
|
|
|
|
M |
|
D |
|
Y |
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
SMEAR |
CLINICAL* |
|
|
|
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
*Fill out reverse of form |
|
|
|
|
|
|
|
|
|
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||
6. Hispanic or Latino Origin: 1.Yes 2.No 3.Unknown |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
|
|
|
|
|
EXAMINE FOR: |
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||
7. Sex 1.Male 2.Female |
8. Co. of Residence |
|
|
|
|
|
|
|
GC N. MENINGITIDIS GROUP H. INFLUENZAE TYPE |
|
|
||||||||||||||||||||||||||
9.Medicaid ClientYes |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
BORDETELLA PCR BORDETELLA CULTURE |
LEGIONELLA DFA |
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
LEGIONELLA CULTURE REFERENCE ID** |
|
|
|
|
|
|
|
|
|
|||||||
If yes, enter # No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
— |
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
**Describe organism___________________________________________ |
||||||||||||||||||||
Federal Tax No.: ______________________________________ |
|
|
|||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||
|
|
SPECIMEN SOURCE: |
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Send Report To: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
BLOOD CSF |
URINE SPUTUM |
NP |
|
BRONCH WASH |
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
BRONCH LAVAGE BRONCH BRUSH |
THROAT |
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
STERILE BODY FLUID |
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
SPECIAL/ATYPICAL BACTERIOLOGY
LABORATORY REPORT (DO NOT WRITE BELOW)
IDENTIFICATION
GRAM STAIN
HIA
ACTION ON BLOOD TSI: SLANT/BUTT
H2S: TSI BUTT
HS2: LEAD AC
PAPER
OXIDASE
CATALASE
ACETAMIDE
ACETATE
AGAR ADHERENCE BILE ESCULIN BILE SOLUBILITY CETRIMIDE CITRATE COAG.: SLIDE
TUBE
DMSO OXIDASE ESCULIN FLAGELLA FLO GAS/GLU M.R.S.
GELATIN
INDOL
LAP LECITHINASE LITMUS MILK MACCONKEY MOTILITY MR NITRATE NITRITE ONPG
PA PIGMENT PYR PYRUVATE STARCH STRING TEST SS
TECH
UREA VP
3% KOH GEL
DECARBOXYLASES: ARGININE LYSINE ORNITHINE
BASE:
ARABINOSE
FRUCTOSE
GLUCOSE
INULIN
LACTOSE
MALTOSE
MANNITOL
MANNOSE
MELIBIOSE
RAFFINOSE
SALICIN
SORBITOL
SUCROSE
TREHALOSE
TURANOSE
XYLOSE
DATE REPORTED: |
By |
REPORT TELEPHONED TO: |
By |
CULTURE REPORT TO FOLLOW |
|
|
|
FINAL CULTURE REPORT |
By |
|
|
SENT TO CDC FOR FURTHER TESTING |
|
CULTURE SHOWS NO BACTERIAL GROWTH |
NONVIABLE ISOLATE |
GROSSLY MIXED CULTURE
DIRECT FA STAIN FOR _______________________________________
POSITIVE NEGATIVE (DFA STAIN IS A PRESUMPTIVE TEST)
CULTURE FOR BORDETELLA |
POSITIVE |
NEGATIVE |
CULTURE FOR LEGIONELLA |
POSITIVE |
NEGATIVE |
PCR FOR BORDETELLA |
POSITIVE |
NEGATIVE |
|
|
|
SPECIMEN UNSATISFACTORY: |
_______________________________ |
|
BROKEN/LEAKED IN TRANSIT |
SPECIMEN UNLABELED |
|
QUANTITY INSUFFICIENT SPECIMEN IMPROPERLY PREPARED
NO SPECIMEN |
|
|
FORM IMPROPERLY PREPARED |
||
|
|
|
|
|
|
%NACL: 0% |
6% |
6.5% |
8% |
10% |
|
GROWTH TEMP.: |
10C |
25C |
35C |
42C |
45C |
SEROLOGICAL GROUP |
GROWTH ON MEDIA: |
ANTIBIOTIC DISCS: |
|||
|
|
CA |
|
|
VANCOMYCIN |
|
|
SBA |
|
|
POLYMYXIN B |
DNA PROBE |
|
MAC |
|
|
NOVOBIOCIN |
DNASE |
|
GCLT |
|
FURAZOLIDONE |
|
AMYLOSUCRASE |
|
RAB |
|
|
OPTOCHIN |
NUT. AGAR 35C/AIR |
|
|
|
|
COLISTIN |
GONOCHEK |
|
|
|
|
PENICILLIN |
GONOGEN |
|
|
|
|
|
Comments:
DHHS T806 (Revised 10/08) LABORATORY (Review 10/10)
PLEASE PROVIDE THE FOLLOWING CLINICAL OR EPIDEMIOLOGIC INFORMATION
ANY ASSOCIATED ILLNESS____________________________________________________ |
DATE OF ONSET _________________________________ |
PERTINENT CLINICAL FINDINGS________________________________________________ |
SYMPTOMS _____________________________________ |
PREVIOUS LABORATORY RESULTS_____________________________________________ |
______________________________________ |
EPIDEMIOLOGICAL DATA: SINGLE CASE SPORADIC CONTACT EPIDEMIC CARRIER ANIMAL CONTACT ___________
FOREIGN OR DOMESTIC TRAVEL? WHERE? _____________________________ WHEN? (WITHIN LAST YEAR ) _____________________________
OTHER _______________________________________________________________________________________________________________________
INSTRUCTIONS
PURPOSE: Isolation, identiication, conirmation, further studies of
PREPARATION: Collect specimen following instructions in SCOPE, using recommended collection kits. Label each specimen tube, subculture, or smear with patient's name and your laboratory number if appropriate. Fill out this form and send in appropriate mailer with the specimen to State Labo- ratory of Public Health. Place form in outer container. Do not send without label (patient name) on specimen or without form. Forms must be printed from Web site.
PREPARATION OF FORM: Left Upper Portion of Form. Item 1. Enter patient's name, last name irst, irst name, and middle initial or maiden name initial, if female. Item 2. Enter patient's social security number. This is the identifying number for that patient. If the patient has no social security number, please indicate on form and include submitter laboratory/medical record number. Item 3. Enter patient's home address on lines immediately
Right Upper Portion of Form. Specimen Type: Check appropriate box. Date Specimen Collected: Enter date as indicated. Examine For: Suspected disease or type examination required. Specimen Source: Check appropriate box. Symptoms/Epidemiological Information: Check appropriate box(es). Provide any further information listed at top of this page.
Do not write in space below “Laboratory Report.”
DISPOSITION: This form may be destroyed in accordance with Standard 5, Patient Clinical Records, of the Records Disposition Schedule published by the N.C. Division of Archives and History.
DHHS T806 (Revised 10/08) LABORATORY (Review 10/10)