
aesap alabama can be filled in online without difficulty. Just use FormsPal PDF editing tool to finish the job promptly. FormsPal development team is ceaselessly working to improve the editor and make it much easier for users with its extensive functions. Enjoy an ever-improving experience now! Getting underway is simple! Everything you should do is stick to these easy steps below:
Step 1: Firstly, open the editor by clicking the "Get Form Button" at the top of this site.
Step 2: Using our advanced PDF tool, you're able to do more than merely fill in forms. Try each of the functions and make your forms appear great with custom text incorporated, or modify the file's original input to perfection - all comes with an ability to incorporate stunning photos and sign the document off.
This PDF doc needs specific details; to guarantee consistency, please make sure to take note of the subsequent guidelines:
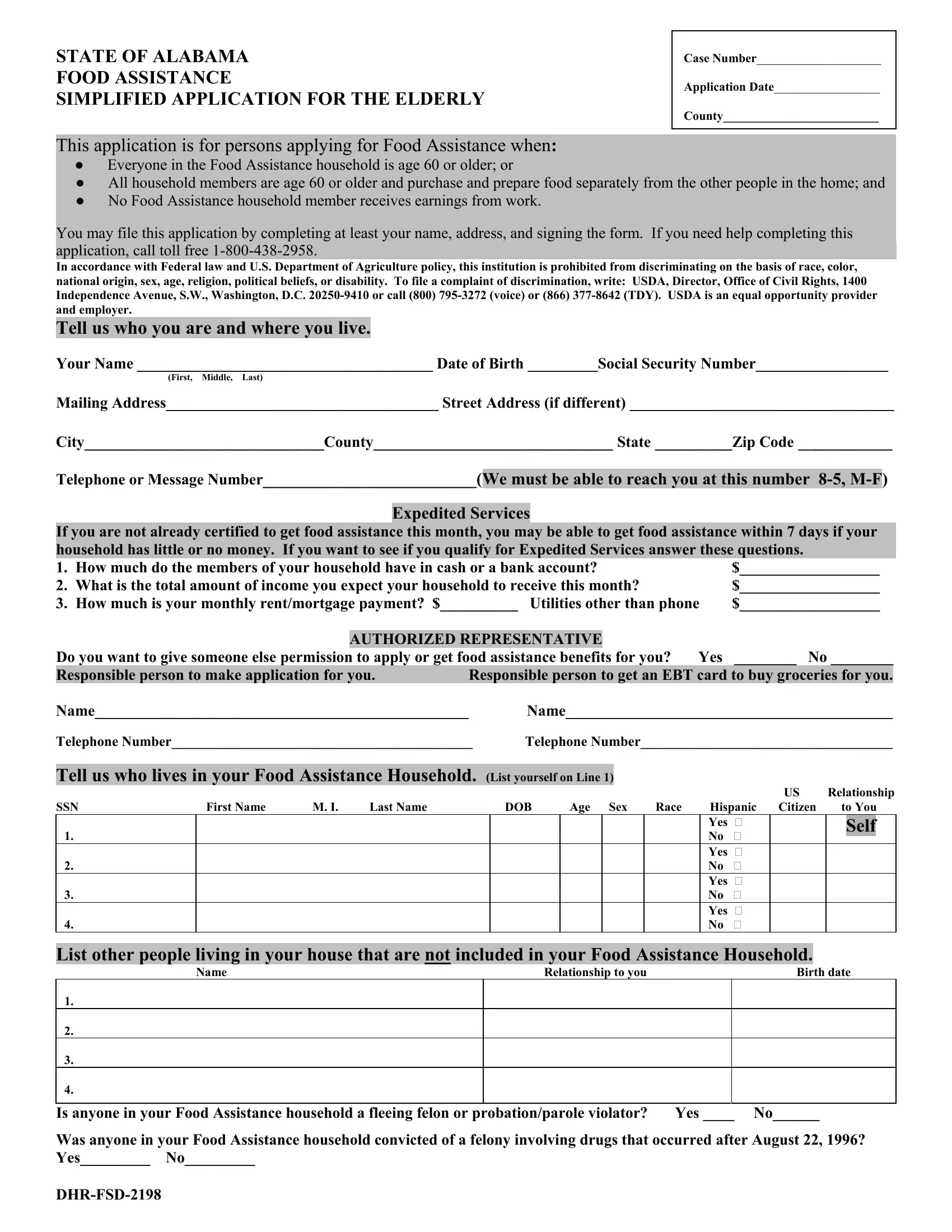
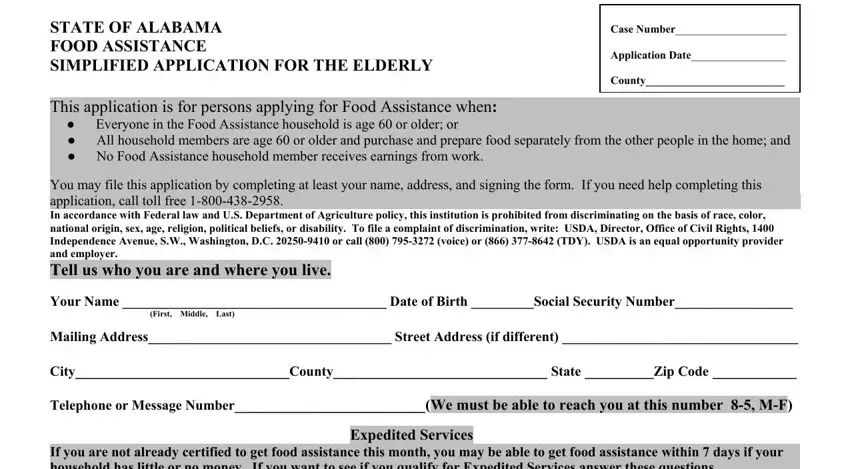
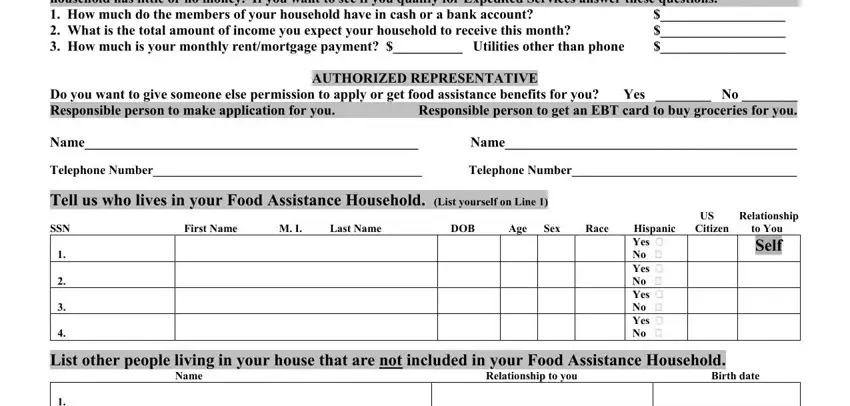
1. To begin with, when filling out the aesap alabama, beging with the page with the following blank fields:
2. The subsequent stage is to submit these fields: If you are not already certified, AUTHORIZED REPRESENTATIVE, Do you want to give someone else, US Relationship, Yes No Yes No Yes No Yes No, and List other people living in your.
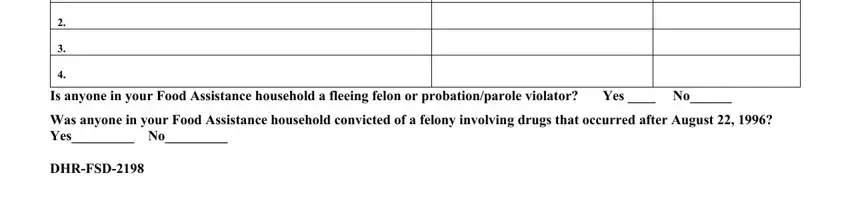
3. This 3rd step is usually fairly easy, Is anyone in your Food Assistance, Was anyone in your Food Assistance, and DHRFSD - these fields has to be filled out here.
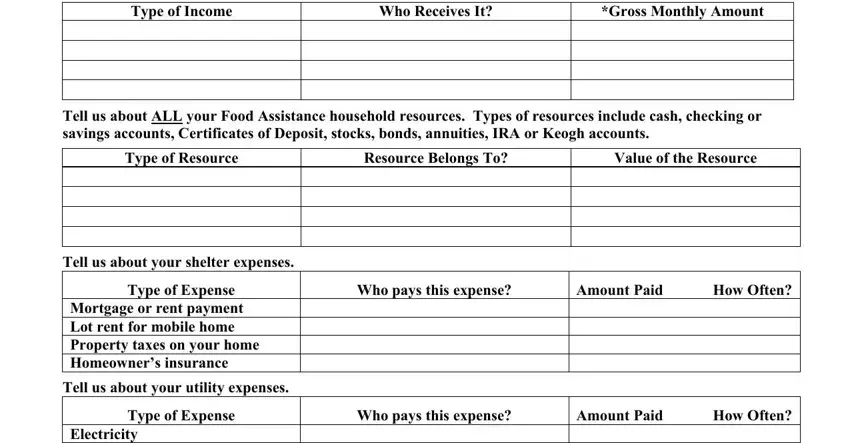
4. This part arrives with the next few empty form fields to type in your information in: Type of Income, Who Receives It, Gross Monthly Amount, Tell us about ALL your Food, Type of Resource, Resource Belongs To, Value of the Resource, Tell us about your shelter expenses, Type of Expense, Mortgage or rent payment Lot rent, Tell us about your utility expenses, Who pays this expense, Amount Paid How Often, Type of Expense, and Who pays this expense.
5. This form must be wrapped up by dealing with this part. Below there can be found a full set of fields that have to be filled out with correct information to allow your document usage to be accomplished: Electricity Gas Water Garbage, Amount Paid How Often, Do you have an Air Conditioner Yes, Have you received Low Income Home, Yes No If yes when, Does anyone in your Food, Example prescriptions doctor, Medical Expense, Monthly Amount, Medical Expense, Monthly Amount, Does anyone in your Food, living in your home Yes No If yes, and Please read and sign this.
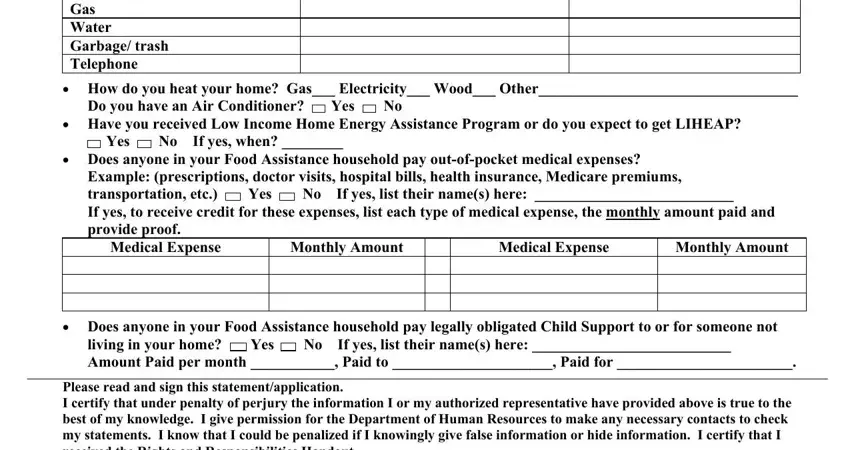
Be very mindful when filling out Have you received Low Income Home and Please read and sign this, since this is where a lot of people make mistakes.
Step 3: After you've reread the details you given, click "Done" to conclude your FormsPal process. Find your aesap alabama after you sign up for a free trial. Quickly get access to the pdf form inside your FormsPal cabinet, with any modifications and adjustments all saved! We don't share or sell the information that you type in while completing forms at FormsPal.