
Any time you desire to fill out MiSDU, you won't need to download and install any sort of programs - simply try our online PDF editor. To retain our editor on the cutting edge of efficiency, we work to put into operation user-oriented capabilities and improvements regularly. We are at all times happy to get feedback - assist us with reshaping how you work with PDF documents. Here is what you would have to do to begin:
Step 1: Firstly, access the editor by clicking the "Get Form Button" above on this page.
Step 2: With our state-of-the-art PDF file editor, you may do more than just fill out blank fields. Try all of the features and make your forms look perfect with customized textual content added, or tweak the file's original input to excellence - all that accompanied by the capability to insert stunning photos and sign it off.
Be mindful when filling in this form. Ensure every single blank is filled out accurately.
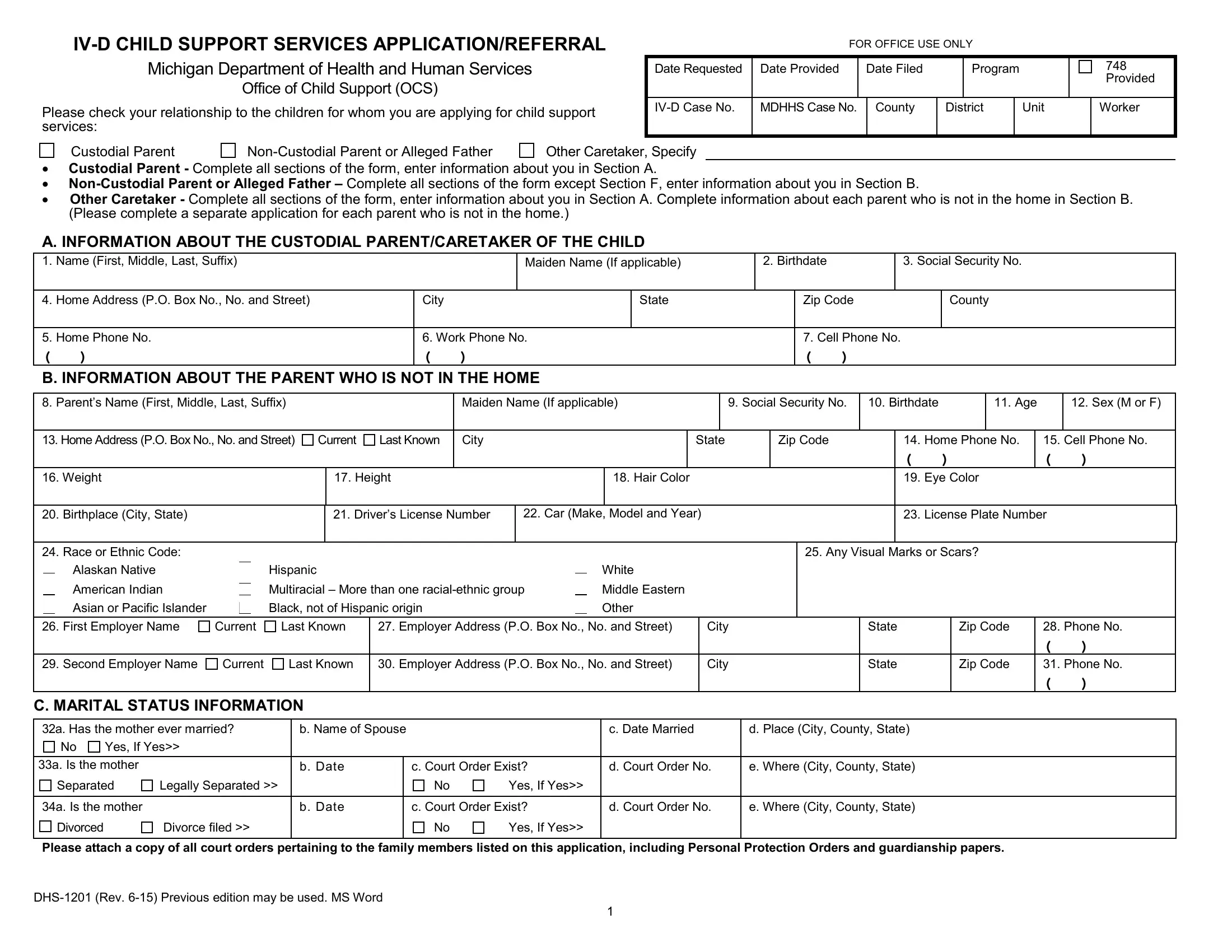
1. You need to fill out the MiSDU correctly, hence be careful when filling in the areas that contain all of these blank fields:
2. After finishing the previous part, go to the subsequent stage and fill in the essential details in all these blanks - American Indian, Asian or Pacific Islander, Black not of Hispanic origin, Multiracial More than one, Middle Eastern, Other, First Employer Name, Current, Last Known, Employer Address PO Box No No and, City, Second Employer Name, Current, Last Known, and Employer Address PO Box No No and.
Always be extremely mindful while completing Middle Eastern and Current, because this is the part in which many people make mistakes.
3. The following step is about D INFORMATION ABOUT CHILDREN Child, e City County State of Birth, g When and where did the mother, b Birthdate, c Social Security Number, d Sex M or F, f Who paid for the birth of child, Date, City, County, State, h Has the father completed a, Yes, Date, and City - fill in all of these fields.
4. The next subsection will require your input in the subsequent parts: h Has the father completed a, Date, City, County, State, CHILDS HEALTH CARE COVERAGE, a Policy Holders Name, b Health Care Company Name, c Coverage Type, d Policy or Group No, Child Three, a Childs Full Name First Middle, e City County State of Birth, g When and where did the mother, and PPO. Be sure to give all of the required info to go onward.
5. Last of all, this final part is what you need to wrap up prior to closing the PDF. The fields in this case are the next: E GENERAL INFORMATION, I believe that disclosure of my, Yes, Yes, I have received or I am currently, If yes when, Where, Yes, If yes when, Where, I am currently receiving Food, Yes, Child Development and Care CDC, Yes, and F ACKNOWLEDGEMENT FOR CUSTODIAL.
Step 3: Ensure the details are accurate and then click "Done" to complete the task. Sign up with FormsPal right now and immediately gain access to MiSDU, ready for downloading. All alterations you make are kept , helping you to change the pdf later on if needed. At FormsPal.com, we do everything we can to make sure your details are kept protected.