
You may complete oral nutrition form 3125 without difficulty with the help of our PDFinity® PDF editor. The tool is consistently updated by our team, receiving new awesome features and becoming better. With a few simple steps, it is possible to start your PDF editing:
Step 1: Just press the "Get Form Button" above on this site to get into our form editor. Here you will find everything that is necessary to fill out your file.
Step 2: With our advanced PDF editor, you'll be able to do more than just complete blank form fields. Express yourself and make your docs seem professional with custom textual content incorporated, or fine-tune the original content to excellence - all supported by the capability to add almost any pictures and sign the document off.
As for the fields of this specific form, here is what you want to do:
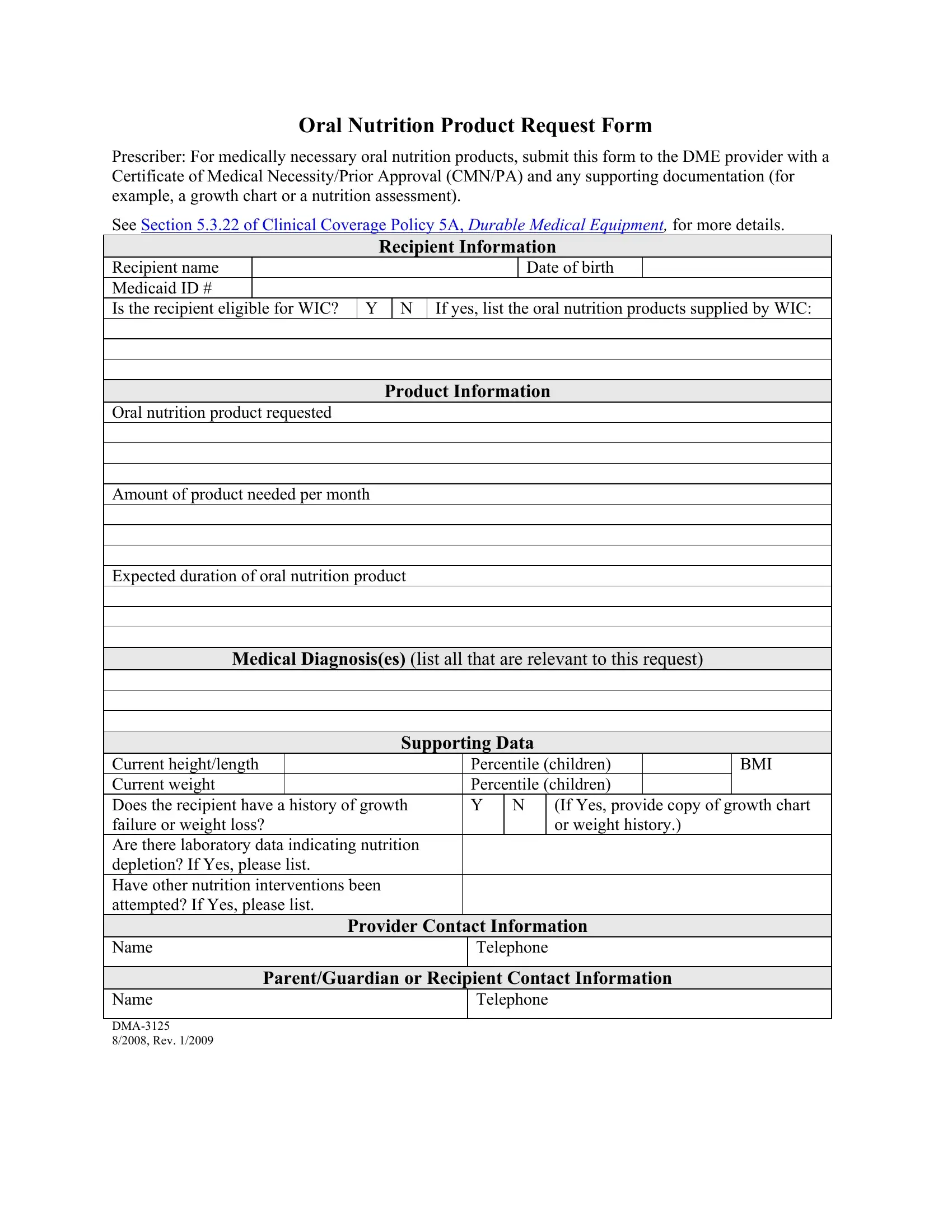
1. Fill out your oral nutrition form 3125 with a group of essential blanks. Gather all of the necessary information and be sure there's nothing neglected!
Step 3: Revise the information you've entered into the blank fields and then click the "Done" button. Try a free trial subscription at FormsPal and get direct access to oral nutrition form 3125 - download, email, or edit inside your FormsPal account. FormsPal guarantees your information privacy with a protected method that in no way records or shares any type of private data used. You can relax knowing your docs are kept confidential each time you use our editor!