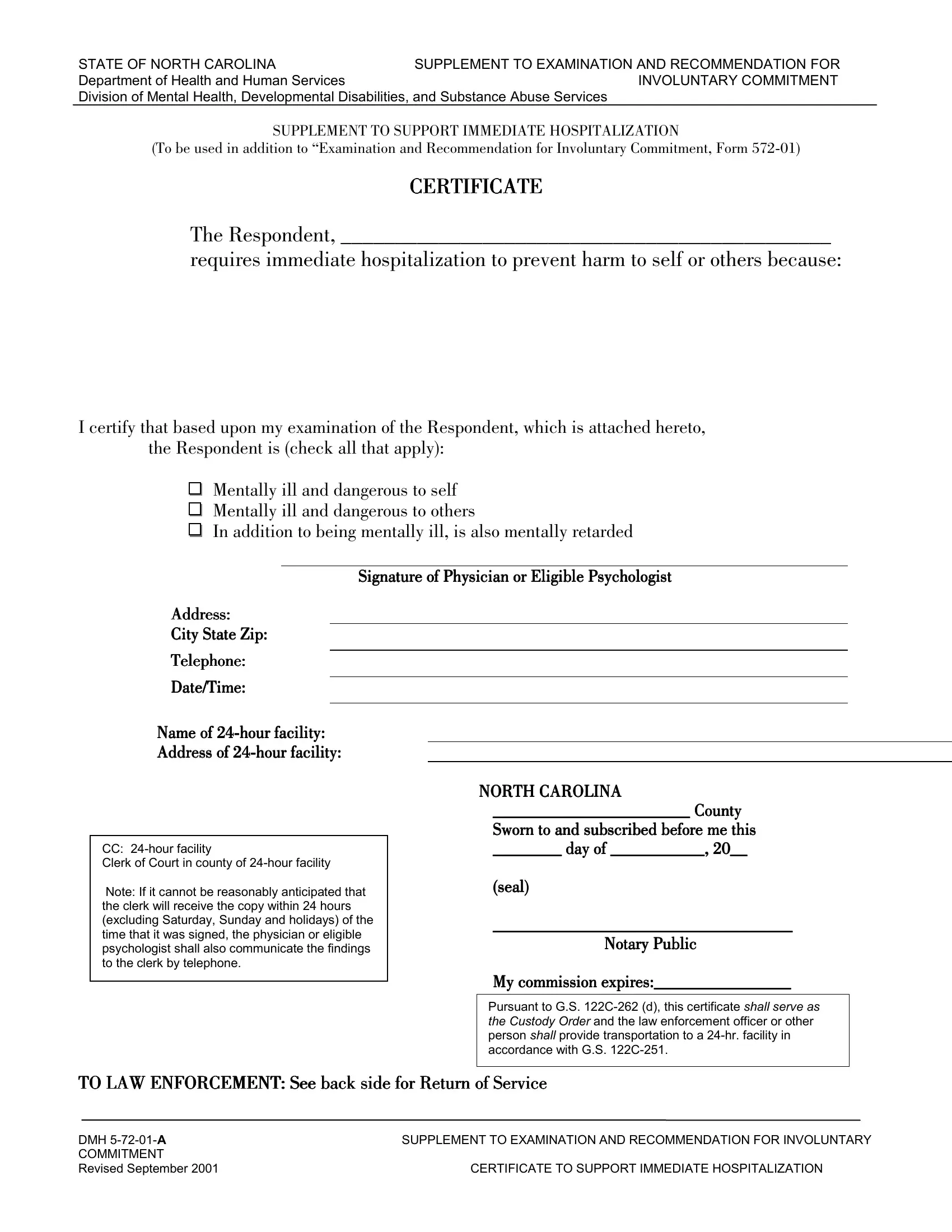
In North Carolina, the delicate balance between personal freedom and public safety is navigated with tools like the DMH 5-72-01 A form, a critical instrument in the process of involuntary commitment. This form acts as a supplement to the Examination and Recommendation for Involuntary Commitment, providing a legal structure for immediate hospitalization when an individual poses a significant risk to themselves or others due to mental illness. It is meticulously designed to ensure that the process adheres to both the state's legal standards and the needs of the community for protection. Physicians or eligible psychologists complete the certificate after a thorough evaluation, affirming the necessity for rapid intervention. The form also includes sections for law enforcement and transportation directives, ensuring swift action while maintaining the dignity and rights of the respondent. Moreover, it facilitates communication with the court system, specifically the clerk of the court in the county where the 24-hour facility is located, ensuring a seamless legal process. This form embodies a crucial intersection of healthcare, law enforcement, and judicial systems, aiming to provide care for individuals in crisis while safeguarding community welfare.
| Question | Answer |
|---|---|
| Form Name | Form Dmh 5 72 01 A |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | 122C-251, HOSPITALIZATION, Disabilities, DMH |
STATE OF NORTH CAROLINA |
SUPPLEMENT TO EXAMINATION AND RECOMMENDATION FOR |
Department of Health and Human Services |
INVOLUNTARY COMMITMENT |
Division of Mental Health, Developmental Disabilities, and Substance Abuse Services
SUPPLEMENT TO SUPPORT IMMEDIATE HOSPITALIZATION
(To be used in addition to “Examination and Recommendation for Involuntary Commitment, Form
CERTIFICATE
The Respondent, _____________________________________________
requires immediate hospitalization to prevent harm to self or others because:
I certify that based upon my examination of the Respondent, which is attached hereto, the Respondent is (check all that apply):
Mentally ill and dangerous to self
Mentally ill and dangerous to others
In addition to being mentally ill, is also mentally retarded
Signature of Physician or Eligible Psychologist
Address:
City State Zip:
Telephone:
Date/Time:
Name of
Address of
CC:
Clerk of Court in county of
Note: If it cannot be reasonably anticipated that the clerk will receive the copy within 24 hours (excluding Saturday, Sunday and holidays) of the time that it was signed, the physician or eligible psychologist shall also communicate the findings to the clerk by telephone.
NORTH CAROLINA
_______________________ County
Sworn to and subscribed before me this
________ day of ___________, 20__
(seal)
___________________________________
Notary Public
My commission expires:________________
Pursuant to G.S.
TO LAW ENFORCEMENT: See back side for Return of Service
DMH |
SUPPLEMENT TO EXAMINATION AND RECOMMENDATION FOR INVOLUNTARY |
COMMITMENT |
|
Revised September 2001 |
CERTIFICATE TO SUPPORT IMMEDIATE HOSPITALIZATION |
STATE OF NORTH CAROLINA |
SUPPLEMENT TO EXAMINATION AND RECOMMENDATION FOR |
Department of Health and Human Services |
INVOLUNTARY COMMITMENT |
Division of Mental Health, Developmental Disabilities, and Substance Abuse Services
RETURN OF SERVICE
Respondent WAS NOT taken into custody for the following reason:
I certify that this Order was received and served as follows:
Date Respondent Taken into Custody |
Time |
|
|
|
|
|
|
|
|
|
|
|
|
|
AM |
|
|
|
|
|
|
||
|
|
|
|
|
|
|
PM |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Name of |
Date Delivered |
Time Delivered |
|
Date of |
|||
|
|
|
|
Return |
|||
|
|
AM |
|
|
|
||
|
|
|
|
||||
|
|
|
|
|
|||
|
|
PM |
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
Name of Transporting Agency |
Signature of Law Enforcement Official |
|
|
||||
|
|
|
|
|
|
|
|
DMH |
SUPPLEMENT TO EXAMINATION AND RECOMMENDATION FOR INVOLUNTARY |
COMMITMENT |
|
Revised September 2001 |
CERTIFICATE TO SUPPORT IMMEDIATE HOSPITALIZATION |