You'll find nothing challenging about filling out the 2020 nys opt out letter once you begin using our PDF tool. Following these basic steps, you will get the ready PDF document within the minimum period possible.
Step 1: Press the "Get Form Now" button to begin.
Step 2: After you've accessed the 2020 nys opt out letter edit page, you'll see all functions you can use regarding your file at the upper menu.
Type in the details requested by the system to complete the form.
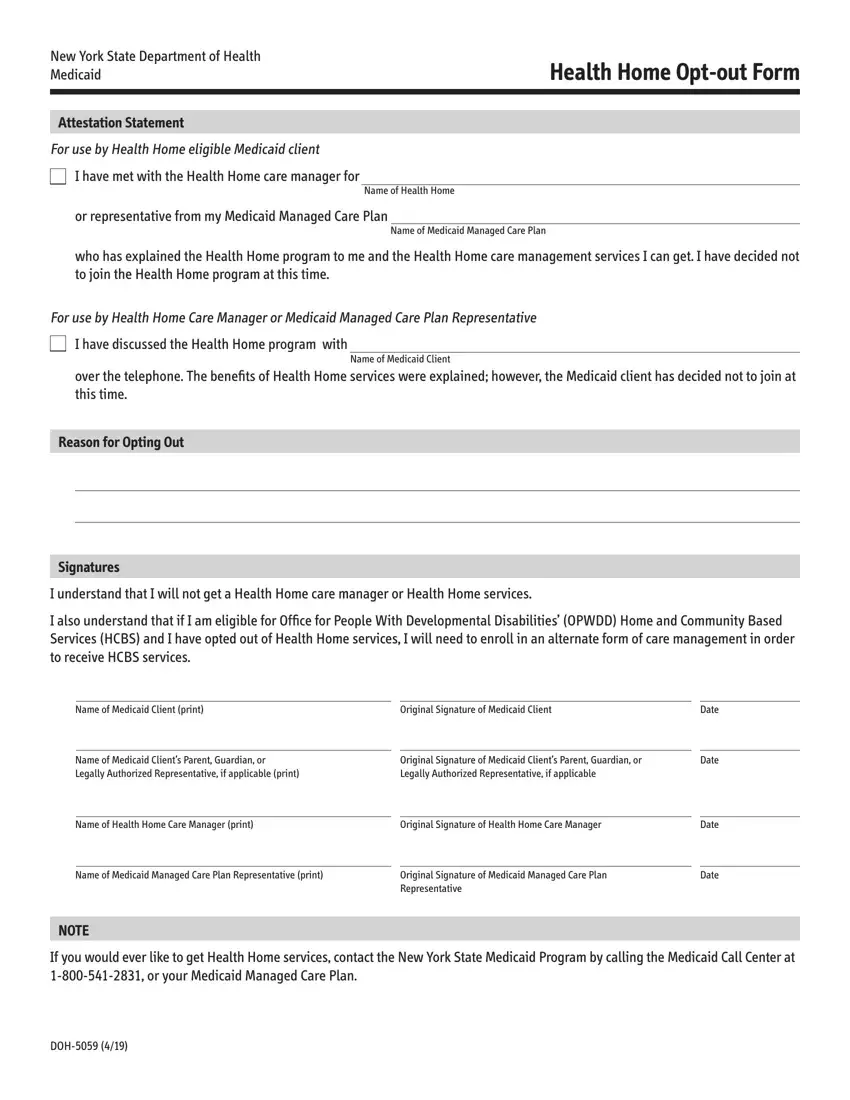
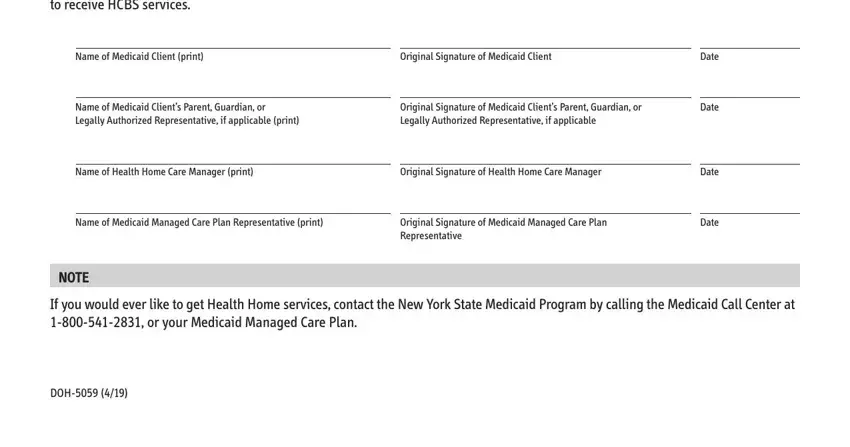
In the part I also understand that if I am, Name of Medicaid Client print, Original Signature of Medicaid, Name of Medicaid Clients Parent, Original Signature of Medicaid, Name of Health Home Care Manager, Original Signature of Health Home, Name of Medicaid Managed Care Plan, Original Signature of Medicaid, Date, Date, Date, Date, NOTE, and If you would ever like to get note the information that the system requests you to do.
Step 3: When you have selected the Done button, your form should be available for upload to any kind of gadget or email address you specify.
Step 4: You should make as many copies of your file as you can to stay away from future complications.
