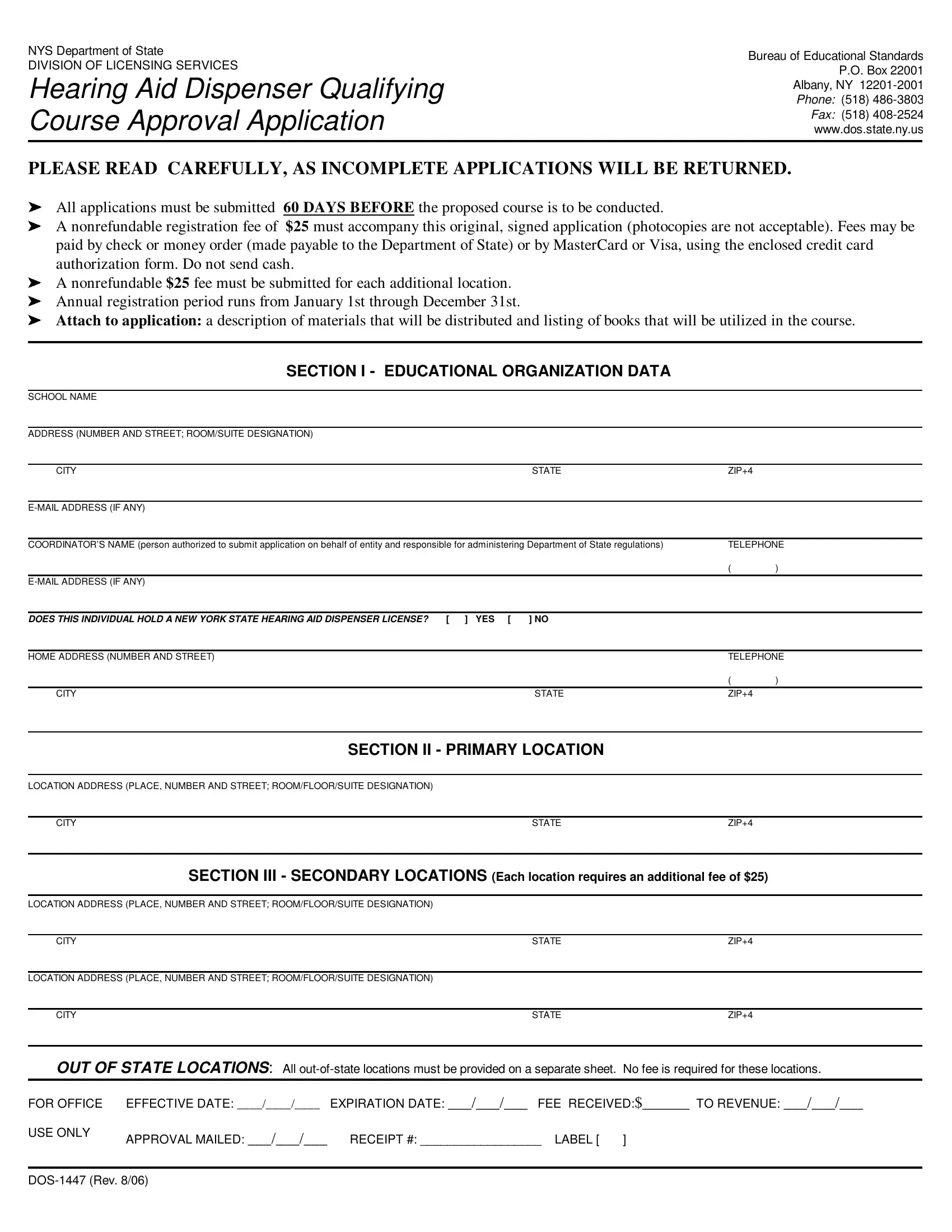
The DOS 1447 form is a vital document for entities within New York State seeking approval to conduct Hearing Aid Dispenser Qualifying Courses, administrated by the Bureau of Educational Standards under the Division of Licensing Services. This comprehensive application requires meticulous attention to detail, as incomplete submissions are subject to return. A notable aspect of this process is the mandate that all applications be submitted 60 days prior to the proposed course date, accompanied by a nonrefundable registration fee of $25, alongside a similar fee for each additional course location. Payment can be made via check, money order, or credit card, with explicit instructions against sending cash. The form delves into various sections that encompass educational organization data, detailing the school's name, address, the coordinator responsible for adhering to Department of State regulations, and whether this individual holds a valid New York State Hearing Aid Dispenser License. Further information is sought on primary and secondary locations, the organizational structure—whether it be a college, individual ownership, partnership, or corporation—and requires disclosure of any criminal convictions or past issues with licenses or permits among owners or key personnel. All instructors must also be registered with the Department, and the application concludes with a sworn affirmation of the accuracy and truthfulness of the provided information, underlining the seriousness of the application in maintaining high educational and ethical standards in the field of hearing aid dispensation.
| Question | Answer |
|---|---|
| Form Name | Form Dos 1447 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | 1447 a online nys hearing aide dispenser courses form |
NYS Department of State |
Bureau of Educational Standards |
|
DIVISION OF LICENSING SERVICES |
||
P.O. Box 22001 |
||
|
Hearing Aid Dispenser Qualifying |
Phone: (518) |
|
Course Approval Application |
Albany, NY |
|
www.dos.state.ny.us |
||
|
Fax: (518) |
|
|
|
|
PLEASE READ CAREFULLY, AS INCOMPLETE APPLICATIONS WILL BE RETURNED.
All applications must be submitted 60 DAYS BEFORE the proposed course is to be conducted.
A nonrefundable registration fee of $25 must accompany this original, signed application (photocopies are not acceptable). Fees may be paid by check or money order (made payable to the Department of State) or by MasterCard or Visa, using the enclosed credit card authorization form. Do not send cash.
A nonrefundable $25 fee must be submitted for each additional location. Annual registration period runs from January 1st through December 31st.
'Attach to application: a description of materials that will be distributed and listing of books that will be utilized in the course.
SECTION I - EDUCATIONAL ORGANIZATION DATA
SCHOOL NAME
ADDRESS (NUMBER AND STREET; ROOM/SUITE DESIGNATION)
CITY |
STATE |
ZIP+4 |
|
|
|
|
|
|
|
|
|
|
|
||
COORDINATOR’S NAME (person authorized to submit application on behalf of entity and responsible for administering Department of State regulations) |
TELEPHONE |
||
|
|
( |
) |
|
|
|
|
|
|
|
|
DOES THIS INDIVIDUAL HOLD A NEW YORK STATE HEARING AID DISPENSER LICENSE? |
[ ] YES [ ] NO |
|
|
|
|
|
|
HOME ADDRESS (NUMBER AND STREET) |
|
TELEPHONE |
|
|
|
( |
) |
CITY |
STATE |
ZIP+4 |
|
SECTION II - PRIMARY LOCATION
LOCATION ADDRESS (PLACE, NUMBER AND STREET; ROOM/FLOOR/SUITE DESIGNATION)
CITYSTATEZIP+4
SECTION III - SECONDARY LOCATIONS (Each location requires an additional fee of $25)
LOCATION ADDRESS (PLACE, NUMBER AND STREET; ROOM/FLOOR/SUITE DESIGNATION)
CITY |
STATE |
ZIP+4 |
|
|
|
LOCATION ADDRESS (PLACE, NUMBER AND STREET; ROOM/FLOOR/SUITE DESIGNATION) |
|
|
|
|
|
CITY |
STATE |
ZIP+4 |
OUT OF STATE LOCATIONS: All
FOR OFFICE EFFECTIVE DATE: ____/____/____ |
EXPIRATION DATE: ___/___/___ FEE RECEIVED:$______ TO REVENUE: ___/___/___ |
|
USE ONLY |
APPROVAL MAILED: ___/___/___ |
RECEIPT #: __________________ LABEL [ ] |
|
||
Hearing Aid Dispenser Qualifying Course Approval Application |
Page 2 of 2 |
|
|
SECTION IV - TYPE OF EDUCATIONAL ORGANIZATION OWNERSHIP |
|
|
|
Is this organization an accredited College or University? Yes [ ] No* [ ] *If No, Please complete one of the following: |
|
INDIVIDUAL: (Please submit a certified copy of the Trade Name Certificate and complete the following for Owner.)
NAME |
HOME ADDRESS (NUMBER AND STREET) |
|
|
|
|
CITY |
STATE |
ZIP+4 |
PARTNERSHIP: (Please submit a copy of Partnership Agreement and complete the following for all Partners.)
NAME |
HOME ADDRESS (NUMBER AND STREET) |
|
|
|
|
CITY |
STATE |
ZIP+4 |
|
|
|
NAME |
HOME ADDRESS (NUMBER AND STREET) |
|
|
|
|
CITY |
STATE |
ZIP+4 |
CORPORATION: (Please submit a copy of the Certificate of Incorporation and complete the following for all officers and other individuals who own 5% or more of the stock of this corporation. If needed, attach additional sheets.)
NAME |
HOME ADDRESS (NUMBER AND STREET) |
|
|
|
|
CITY |
STATE |
ZIP+4 |
|
|
|
NAME |
HOME ADDRESS (NUMBER AND STREET) |
|
|
|
|
CITY |
STATE |
ZIP+4 |
|
|
|
NAME |
HOME ADDRESS (NUMBER AND STREET) |
|
|
|
|
CITY |
STATE |
ZIP+4 |
Has any owner, partner, owner of 5% or more of the stock of the entity, or individual authorized to submit this application on behalf of the entity been convicted of any crime or offense, other than a minor traffic violation?
[ ] Yes* [ ] No *If Yes, submit a certified copy of each conviction.
Has any license or permit issued to, applied for by any owner, partner, holder of 5% or more of the stock of the entity, or individual authorized to submit this application on behalf of the entity, been denied, suspended or revoked by this state or elsewhere by an y other government or regulatory body?
[ ] Yes* [ ] No *If Yes, please provide details.
Course Instructors:All instructors of approved courses must be registered with the Department of State. Applications for hearing aid dispenser instructor approval are available by request to the Division of Licensing Services, Bureau of Educational Standards. A one time evaluation and filing fee of $25 is required for each instructor’s approval.
I subscribe and affirm under the penalties of perjury that the statements made in this application (including statements made in any accompanying papers) have been examined by me, and to the best of my knowledge and belief, are true and correct.
I understand that any misstatement made on this application for approval could result in an immediate revocation or withdrawal of the recognition of the approval of the entity by the Department of State.
Coordinator Signature X |
|
Date |
|
A $20 fee will be charged for any check returned by a bank |
|