
Using PDF files online is always simple with this PDF editor. Anyone can fill out dot mis data collection form here with no trouble. To keep our editor on the forefront of convenience, we work to implement user-oriented capabilities and enhancements regularly. We're routinely thankful for any feedback - play a pivotal part in revolutionizing PDF editing. All it takes is a couple of simple steps:
Step 1: Open the form inside our editor by hitting the "Get Form Button" above on this page.
Step 2: With this advanced PDF file editor, you could do more than simply fill in blanks. Edit away and make your docs appear high-quality with custom textual content added, or optimize the original input to perfection - all comes with an ability to incorporate just about any graphics and sign the PDF off.
In an effort to complete this form, make certain you provide the required information in each field:
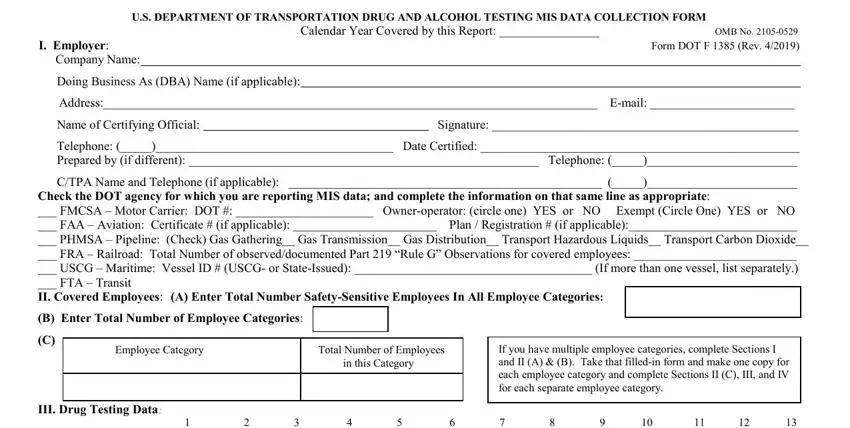
1. Whenever filling in the dot mis data collection form, make sure to incorporate all important fields within its relevant form section. This will help facilitate the work, allowing for your details to be handled quickly and accurately.
2. Once your current task is complete, take the next step – fill out all of these fields - Type of Test, PreEmployment, Random, PostAccident, Reasonable SuspCause, ReturntoDuty, FollowUp, TOTAL, l a t o T, l a u q e d l u o h S s t l u s e, f o m u s e h t, e v i t a g e N d e i f i r e V, s t l u s e R, r o F s t l u s e R, and e v i t i s o P d e i f i r e V with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
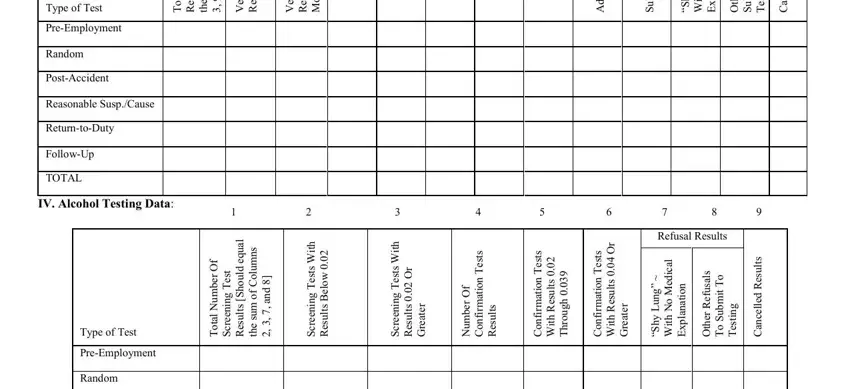
3. In this step, have a look at PostAccident, Reasonable SuspCause, ReturntoDuty, FollowUp, and TOTAL. Each one of these have to be taken care of with greatest accuracy.

Always be very mindful when completing ReturntoDuty and TOTAL, since this is the section where a lot of people make mistakes.
Step 3: Once you've reread the information you filled in, click "Done" to conclude your form. Right after registering a7-day free trial account at FormsPal, you will be able to download dot mis data collection form or send it via email immediately. The PDF will also be at your disposal via your personal cabinet with your each modification. With FormsPal, you'll be able to complete forms without needing to worry about database breaches or data entries being distributed. Our protected software helps to ensure that your private details are kept safely.