
When using the online editor for PDFs by FormsPal, it is possible to fill out or edit Form Dpr Pml 052 here and now. To maintain our tool on the cutting edge of convenience, we strive to put into operation user-oriented capabilities and enhancements on a regular basis. We're routinely glad to receive feedback - join us in revolutionizing PDF editing. Getting underway is simple! Everything you need to do is adhere to the following easy steps down below:
Step 1: First of all, open the pdf tool by clicking the "Get Form Button" above on this page.
Step 2: This editor lets you customize your PDF in a range of ways. Improve it with any text, adjust what's originally in the file, and include a signature - all within the reach of a couple of clicks!
As for the blank fields of this specific form, this is what you should do:
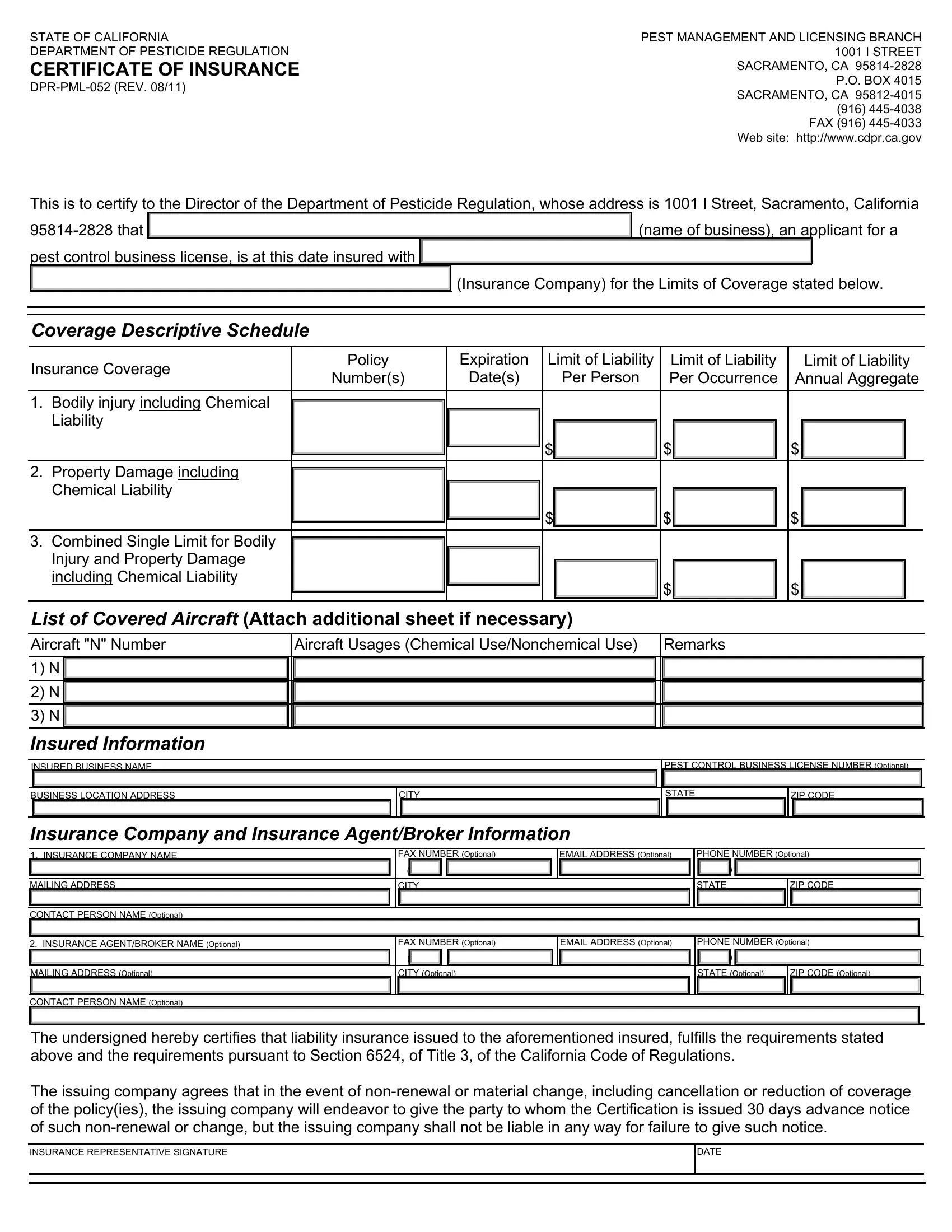
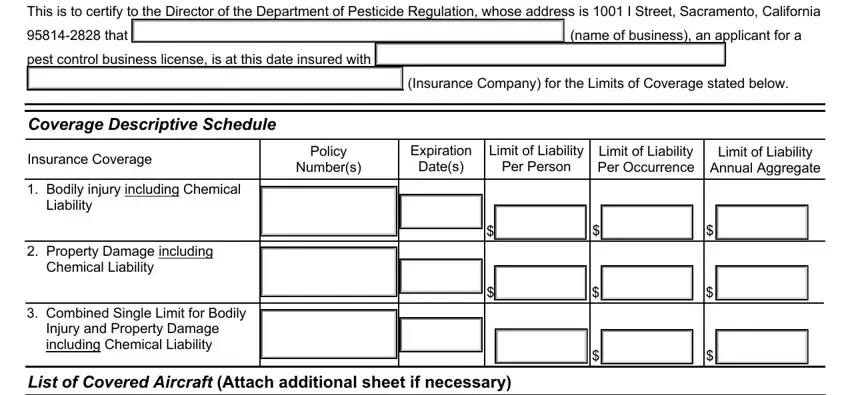
1. You have to fill out the Form Dpr Pml 052 properly, thus pay close attention while filling out the segments containing these specific blank fields:
2. Immediately after this selection of blanks is completed, proceed to enter the applicable information in these - List of Covered Aircraft Attach, Aircraft Usages Chemical, Remarks, Insured Information, INSURED BUSINESS NAME, PEST CONTROL BUSINESS LICENSE, BUSINESS LOCATION ADDRESS, CITY, STATE, ZIP CODE, Insurance Company and Insurance, FAX NUMBER Optional, EMAIL ADDRESS Optional, MAILING ADDRESS, and CONTACT PERSON NAME Optional.
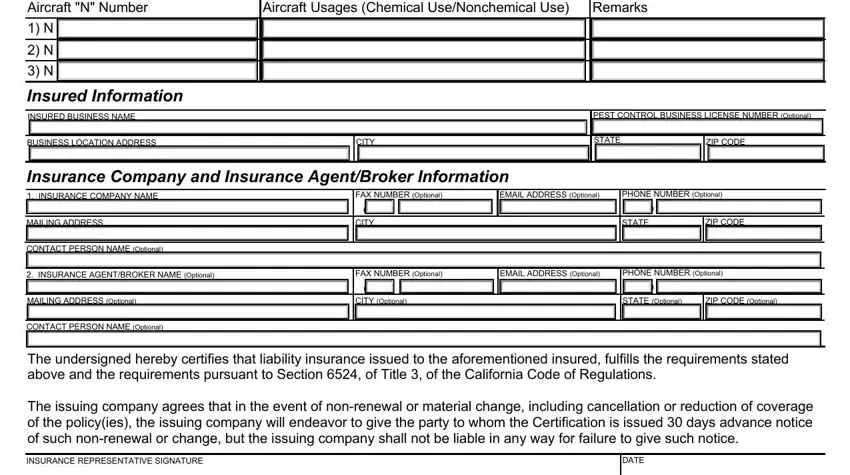
Concerning Aircraft Usages Chemical and EMAIL ADDRESS Optional, make certain you do everything right here. These are certainly the most significant fields in this form.
Step 3: Reread the details you have entered into the blank fields and then hit the "Done" button. Sign up with us right now and immediately access Form Dpr Pml 052, prepared for downloading. All changes you make are kept , so that you can modify the form later anytime. FormsPal guarantees safe form tools without personal data recording or sharing. Feel comfortable knowing that your information is in good hands with us!