

Through the online editor for PDFs by FormsPal, it is easy to fill out or alter dwc 007 texas here. In order to make our editor better and simpler to work with, we constantly design new features, with our users' suggestions in mind. Here is what you'll need to do to start:
Step 1: Click on the "Get Form" button above. It is going to open up our pdf editor so that you could begin filling out your form.
Step 2: With this online PDF file editor, you are able to accomplish more than simply fill in blank fields. Try all the functions and make your documents appear high-quality with customized textual content incorporated, or tweak the file's original content to excellence - all supported by the capability to incorporate your own pictures and sign the file off.
In order to complete this PDF document, ensure you type in the necessary details in each and every field:
1. Whenever filling out the dwc 007 texas, make sure to incorporate all needed blanks within the corresponding form section. It will help facilitate the process, making it possible for your details to be handled fast and correctly.
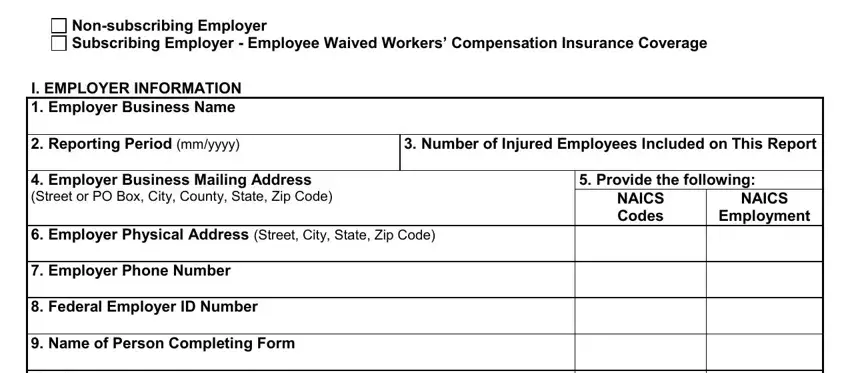
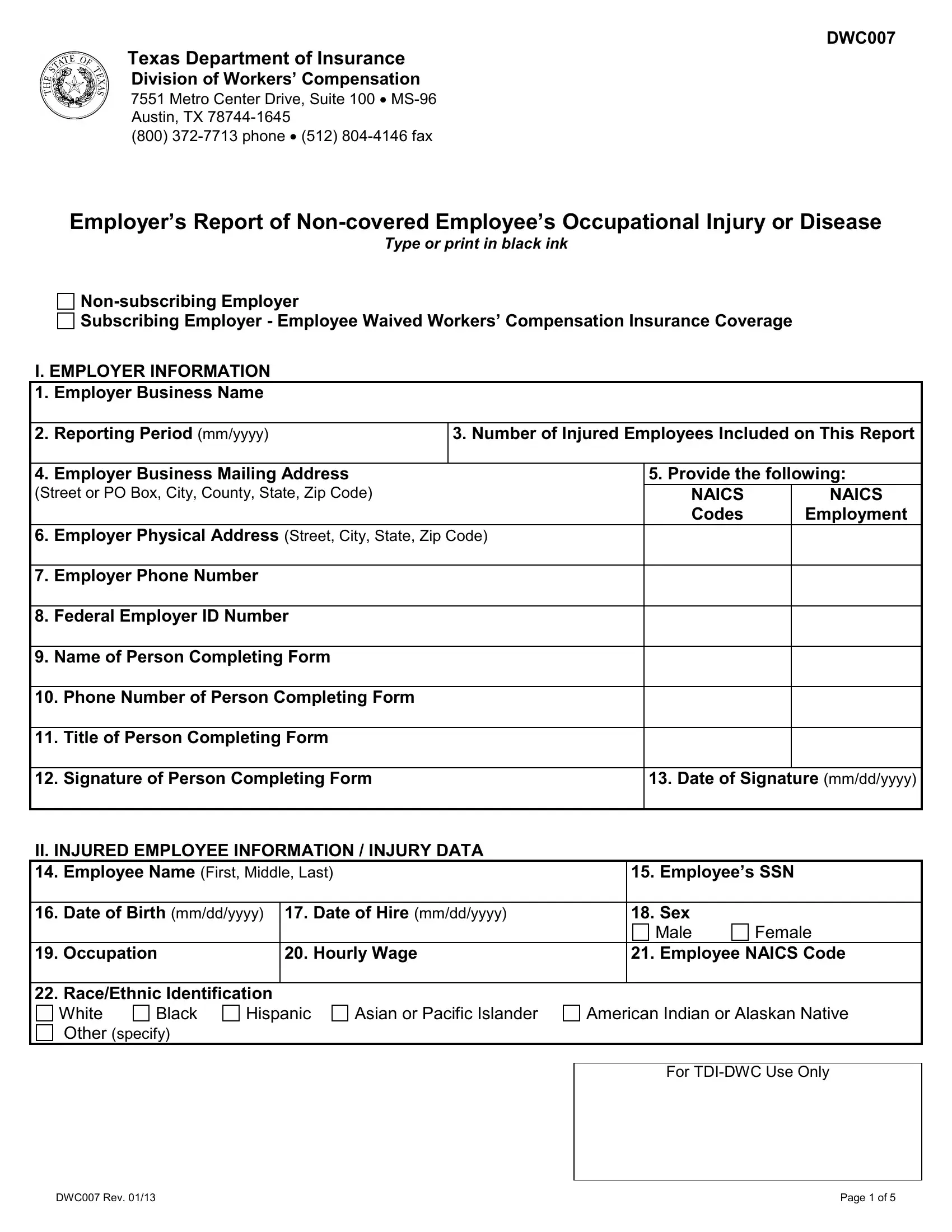
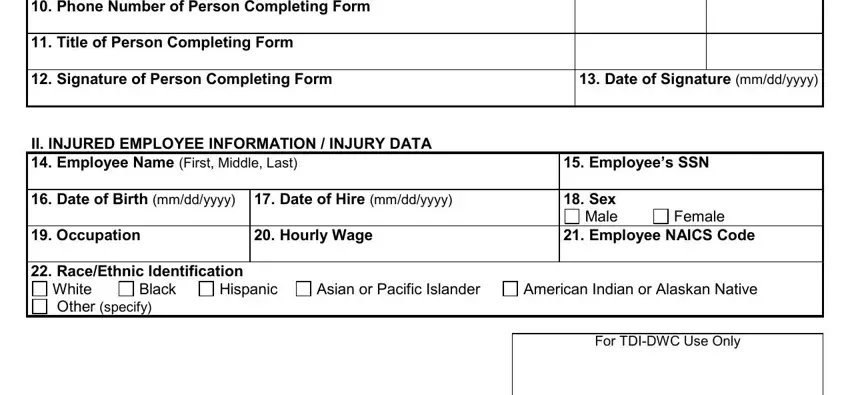
2. Just after filling out the previous part, go to the subsequent step and complete all required details in these blanks - I EMPLOYER INFORMATION Employer, II INJURED EMPLOYEE INFORMATION, Date of Hire mmddyyyy Hourly Wage, Date of Signature mmddyyyy, Employees SSN Sex, Male, Female, Employee NAICS Code, White Black Other specify, Hispanic, Asian or Pacific Islander, American Indian or Alaskan Native, and For TDIDWC Use Only.
Always be extremely mindful while filling out Male and White Black Other specify, since this is the section where most people make errors.
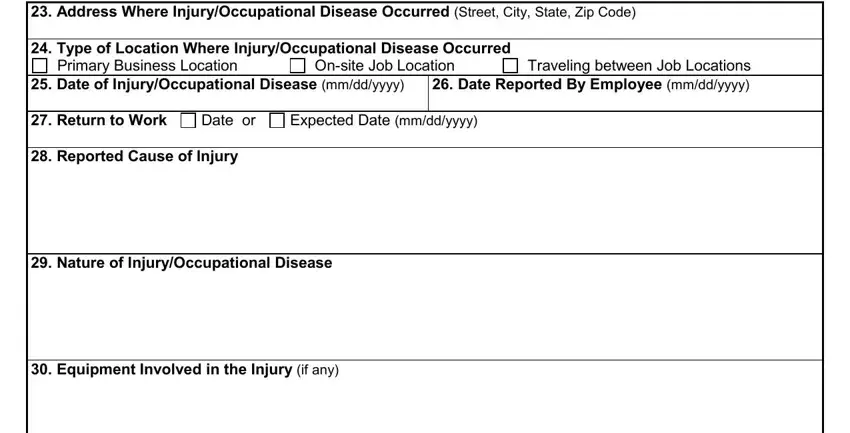
3. Completing Address Where InjuryOccupational, Onsite Job Location, Traveling between Job Locations, Primary Business Location, Date or, and Date of InjuryOccupational is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!
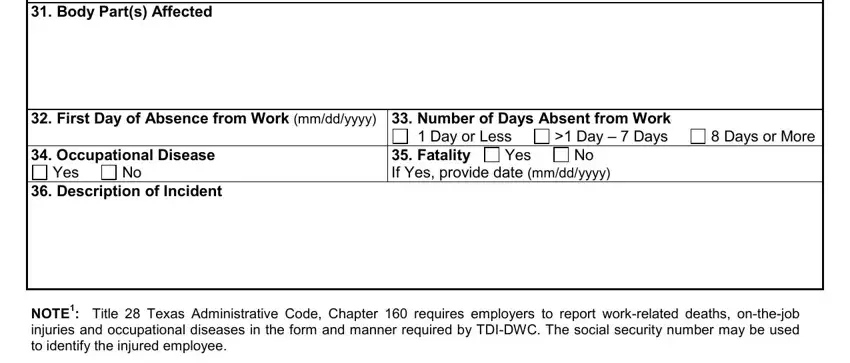
4. Filling out Date of InjuryOccupational, Yes, Number of Days Absent from Work, Day or Less, Day Days, Days or More, Fatality If Yes provide date, Yes, and Description of Incident NOTE is paramount in the next part - be certain to be patient and fill out every single blank area!
5. To wrap up your document, the final part features a number of extra blank fields. Typing in Employers Name Employers FEIN, DWC Rev, For TDIDWC Use Only, and Page of is going to wrap up the process and you'll be done very quickly!

Step 3: Spell-check all the information you've typed into the blank fields and then click the "Done" button. After getting afree trial account at FormsPal, it will be possible to download dwc 007 texas or email it at once. The document will also be available through your personal account page with all your modifications. FormsPal ensures your information privacy by having a secure system that never records or shares any kind of personal information typed in. Feel safe knowing your files are kept safe any time you work with our tools!