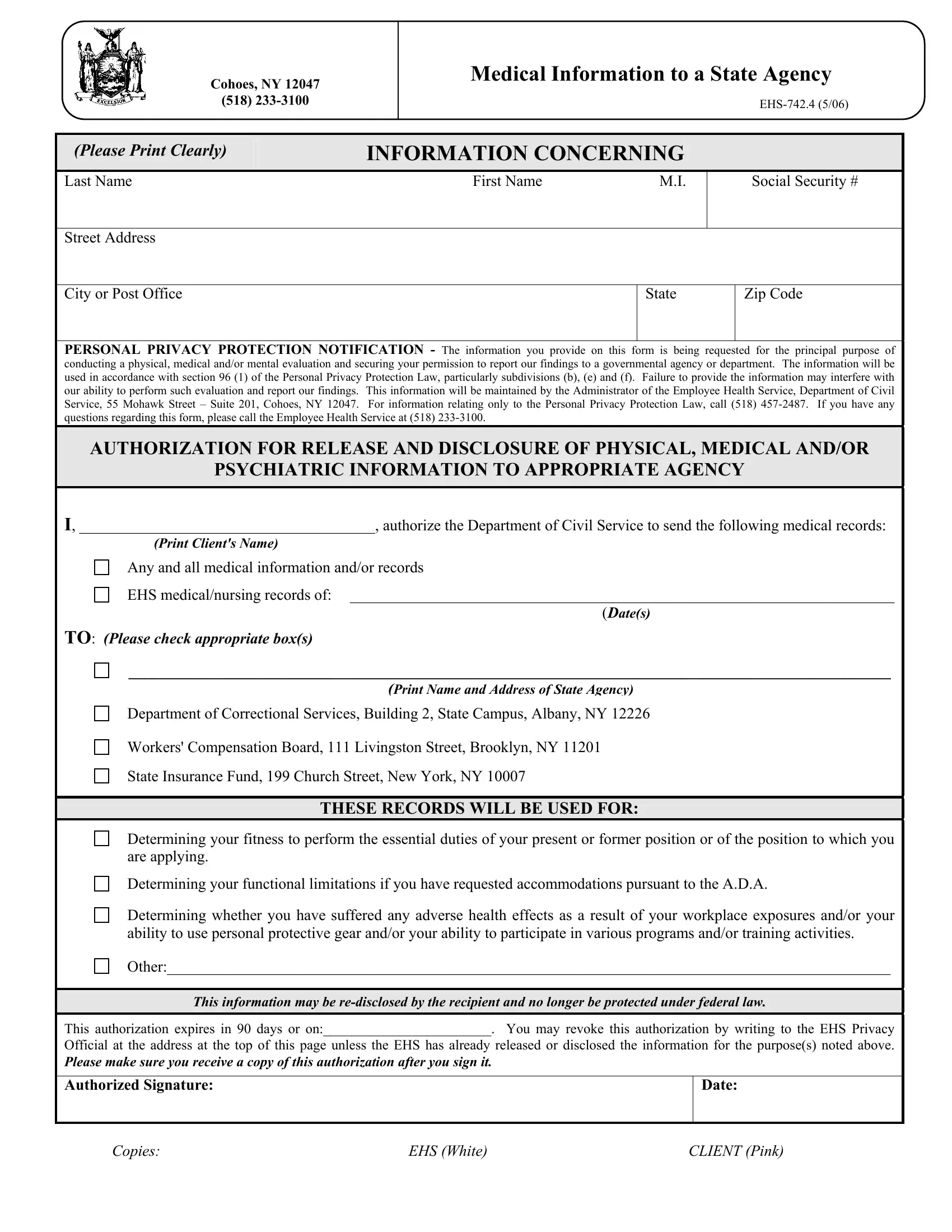
The EHS-742.4 form, issued by the New York State Department of Civil Service's Employee Health Service, plays a crucial role in the management and disclosure of personal medical records within the confines of governmental procedures. Located at 55 Mohawk Street in Cohoes, NY, this entity ensures that individuals grant their explicit consent before any of their medical, psychiatric, or physical information is shared with a state agency, aligning with the Personal Privacy Protection Law. The form serves multiple purposes, including evaluating a person's capability to perform job-related duties, assess any functional limitations for ADA accommodations, or determine the impact of workplace exposures on one's health. With a clear structure, it requests specific details such as personal identification and allows for the allocation of records to various state departments, including the Department of Correctional Services and the State Insurance Fund, among others. The provision within the form that allows for the revocation of consent, the time-bound validity of the authorization, and the emphasis on the individual’s awareness and receipt of a copy upon signing underscore the procedural safeguards put in place to protect the individuals' privacy and rights.
| Question | Answer |
|---|---|
| Form Name | Form Ehs 742 4 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | 55 mohawk street suite 201 cohoes ny 12047, New_York, exposures, ehs 742 4 |
NYS Department of Civil Service
Employee Health Service
55 Mohawk Street – Suite 201
Cohoes, NY 12047
(518)
Authorization for Release and Disclosure of
Medical Information to a State Agency
(Please Print Clearly)
INFORMATION CONCERNING
Last Name |
First Name |
M.I. |
Social Security #
Street Address
City or Post Office
State
Zip Code
PERSONAL PRIVACY PROTECTION NOTIFICATION - The information you provide on this form is being requested for the principal purpose of conducting a physical, medical and/or mental evaluation and securing your permission to report our findings to a governmental agency or department. The information will be used in accordance with section 96 (1) of the Personal Privacy Protection Law, particularly subdivisions (b), (e) and (f). Failure to provide the information may interfere with our ability to perform such evaluation and report our findings. This information will be maintained by the Administrator of the Employee Health Service, Department of Civil Service, 55 Mohawk Street – Suite 201, Cohoes, NY 12047. For information relating only to the Personal Privacy Protection Law, call (518)
AUTHORIZATION FOR RELEASE AND DISCLOSURE OF PHYSICAL, MEDICAL AND/OR
PSYCHIATRIC INFORMATION TO APPROPRIATE AGENCY
I, ______________________________________, authorize the Department of Civil Service to send the following medical records:
(Print Client's Name)
Any and all medical information and/or records
EHS medical/nursing records of: ______________________________________________________________________
(Date(s)
TO: (Please check appropriate box(s)
__________________________________________________________________________________________________
(Print Name and Address of State Agency)
Department of Correctional Services, Building 2, State Campus, Albany, NY 12226
Workers' Compensation Board, 111 Livingston Street, Brooklyn, NY 11201
State Insurance Fund, 199 Church Street, New York, NY 10007
THESE RECORDS WILL BE USED FOR:
Determining your fitness to perform the essential duties of your present or former position or of the position to which you are applying.
Determining your functional limitations if you have requested accommodations pursuant to the A.D.A.
Determining whether you have suffered any adverse health effects as a result of your workplace exposures and/or your ability to use personal protective gear and/or your ability to participate in various programs and/or training activities.
Other:_____________________________________________________________________________________________
This information may be
This authorization expires in 90 days or on:________________________. You may revoke this authorization by writing to the EHS Privacy
Official at the address at the top of this page unless the EHS has already released or disclosed the information for the purpose(s) noted above.
Please make sure you receive a copy of this authorization after you sign it.
Authorized Signature:
Date:
Copies: |
EHS (White) |
CLIENT (Pink) |