Embarking on a career in criminal justice education and training requires thorough preparation and compliance with specific standards. Among the crucial steps for professionals aspiring to enhance their teaching credentials within this field is the completion of the Form F-12. Managed by the Criminal Justice Education and Training Standards Commission, this form is a requisite for individuals seeking probationary general instructor certification, specialized instructor certification in law, medicine, psychology, or professional lecturer certification. The application process underscores the significance of timely submission—specifically within sixty days following the course completion. Additionally, it mandates the provision of detailed educational and practical experience documentation, along with verification of CPR certification for specialized instructors. This process not only evaluates the applicant’s qualifications but also ensures adherence to high standards of instructional quality and ethical conduct. The requirement for a recommendation from a certified school director further validates the applicant’s moral character and capability to train future criminal justice personnel effectively. By navigating through these meticulously designed steps, applicants are better positioned to contribute significantly to the field of criminal justice education and training.
| Question | Answer |
|---|---|
| Form Name | Form F 12 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | f12 form, Raleigh, F-12, form f12 |
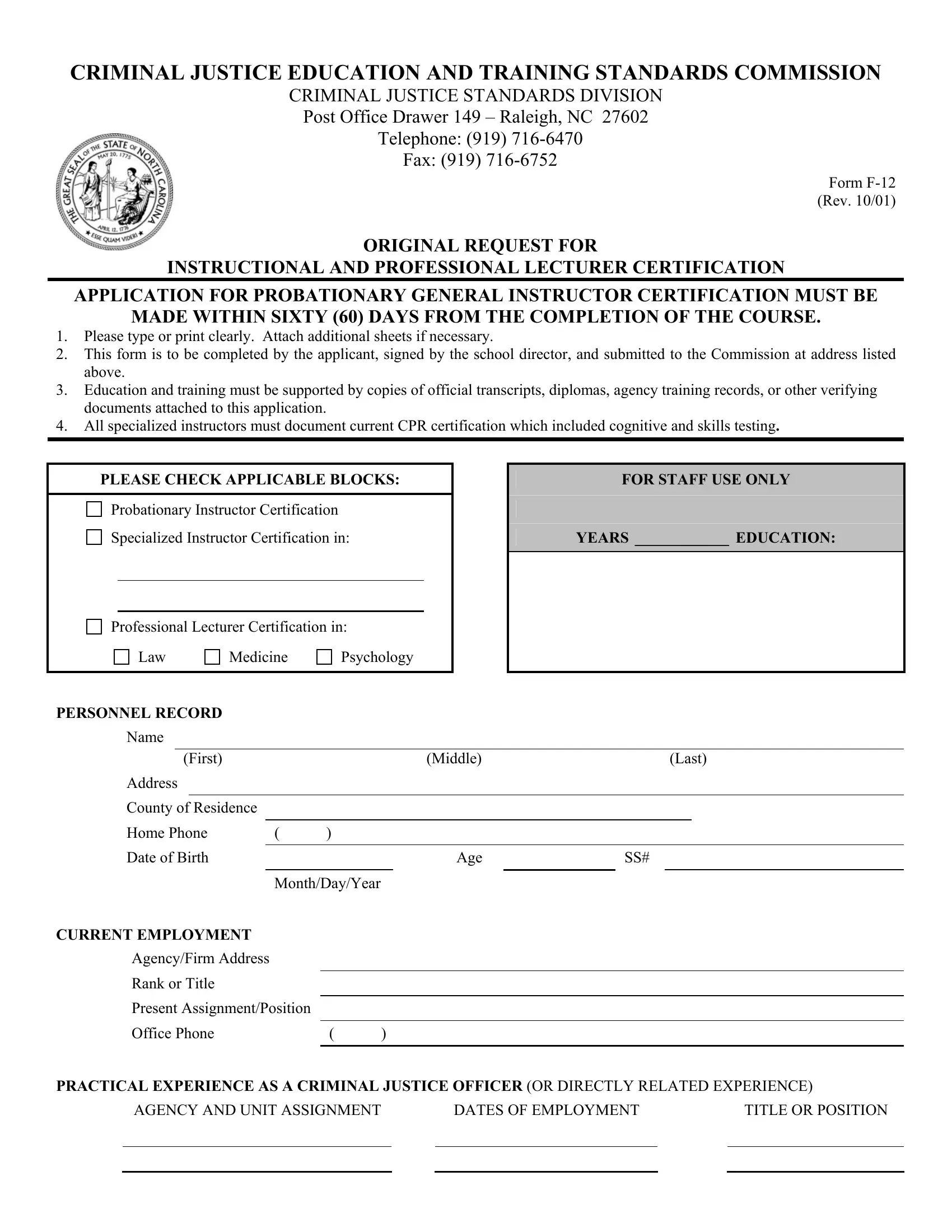
CRIMINAL JUSTICE EDUCATION AND TRAINING STANDARDS COMMISSION
CRIMINAL JUSTICE STANDARDS DIVISION
Post Office Drawer 149 – Raleigh, NC 27602
Telephone: (919)
Fax: (919)
Form
ORIGINAL REQUEST FOR
INSTRUCTIONAL AND PROFESSIONAL LECTURER CERTIFICATION
APPLICATION FOR PROBATIONARY GENERAL INSTRUCTOR CERTIFICATION MUST BE
MADE WITHIN SIXTY (60) DAYS FROM THE COMPLETION OF THE COURSE.
1.Please type or print clearly. Attach additional sheets if necessary.
2.This form is to be completed by the applicant, signed by the school director, and submitted to the Commission at address listed above.
3.Education and training must be supported by copies of official transcripts, diplomas, agency training records, or other verifying documents attached to this application.
4.All specialized instructors must document current CPR certification which included cognitive and skills testing.
PLEASE CHECK APPLICABLE BLOCKS:
Probationary Instructor Certification
Specialized Instructor Certification in:
Professional Lecturer Certification in:
Law Medicine Psychology
PERSONNEL RECORD
FOR STAFF USE ONLY
YEARS ____________ EDUCATION:
Name
(First) |
|
|
(Middle) |
|
|
(Last) |
||
Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
County of Residence |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Home Phone |
( |
) |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Date of Birth |
|
|
Age |
|
SS# |
|||
|
|
|
|
|
|
|
|
|
|
|
Month/Day/Year |
|
|
|
|
||
CURRENT EMPLOYMENT
Agency/Firm Address
Rank or Title
Present Assignment/Position
Office Phone |
( |
) |
|
|
|
PRACTICAL EXPERIENCE AS A CRIMINAL JUSTICE OFFICER (OR DIRECTLY RELATED EXPERIENCE)
AGENCY AND UNIT ASSIGNMENT |
|
DATES OF EMPLOYMENT |
|
TITLE OR POSITION |
|
|
|
|
|
|
|
|
|
|
“The Social Security Number is used to make positive identification of application and/or law enforcement personnel. DISCLOSURE IS VOLUNTARY. However, failure to provide this information may result in a delay in the processing of application materials and may result in inaccurate records being assigned to you.”
COMMISSION ACCREDITED GENERAL AND/OR SPECIFIC INSTRUCTOR TRAINING (OR EQUIVALENT INSTRUCTOR TRAINING)
SCHOOL NAME AND COURSE TITLE |
|
COURSE LENGTH (Hours) |
|
DATE COMPLETED |
|
|
|
|
|
|
|
|
|
|
EDUCATION
NAME OF HIGH SCHOOL |
|
DATES ATTENDED |
|
DIPLOMA? (YES/NO) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
COMMUNITY OR JUNIOR COLLEGE |
|
DATES ATTENDED |
|
DEGREE/HOURS |
|
|
|
|
|
|
|
|
|
|
UNIVERSITY OR COLLEGE |
|
DATES ATTENDED |
|
DEGREE/HOURS |
|
|
|
|
|
|
|
|
|
|
ATTESTATION
CERTIFY THAT THE INFORMATION CONTAINED IN THIS APPLICATION IS TRUE AND CORRECT TO THE BEST OF MY KNOWLEDGE. I ACKNOWLEDGE THAT ANY OMISSION, FALSIFICATION OR MISREPRESENTATION OF THE INFORMATION PROVIDED ABOVE MAY RESULT IN CERTIFICATION BEING DENIED, SUSPENDED, OR REVOKED BY THE COMMISSION.
(DATE) |
(SIGNATURE OF APPLICANT) |
RECOMMENDATION
IT IS RECOMMENDED THAT THE CERTIFICATE REQUESTED BE AWARDED. TO THE BEST OF MY KNOWLEDGE AND BELIEF THE APPLICANT IS OF GOOD MORAL CHARACTER AND HAS THE DESIRE AND THE ABILITY TO PROVIDE EFFECTIVE INSTRUCTION FOR CRIMINAL JUSTICE PERSONNEL.
This the |
|
Day of |
|
20, |
|
. |
(Signature of CERTIFIED) School Director |
(Name of Accredited School) |
Department/Agency and Complete Address