
With the online editor for PDFs by FormsPal, you can easily complete or edit WNL here. The tool is constantly maintained by us, getting cool functions and growing to be greater. To get the ball rolling, take these simple steps:
Step 1: Open the PDF file inside our tool by pressing the "Get Form Button" at the top of this page.
Step 2: The tool enables you to modify PDF documents in a variety of ways. Transform it by adding personalized text, correct existing content, and place in a signature - all within several mouse clicks!
It's an easy task to finish the document following this practical tutorial! This is what you must do:
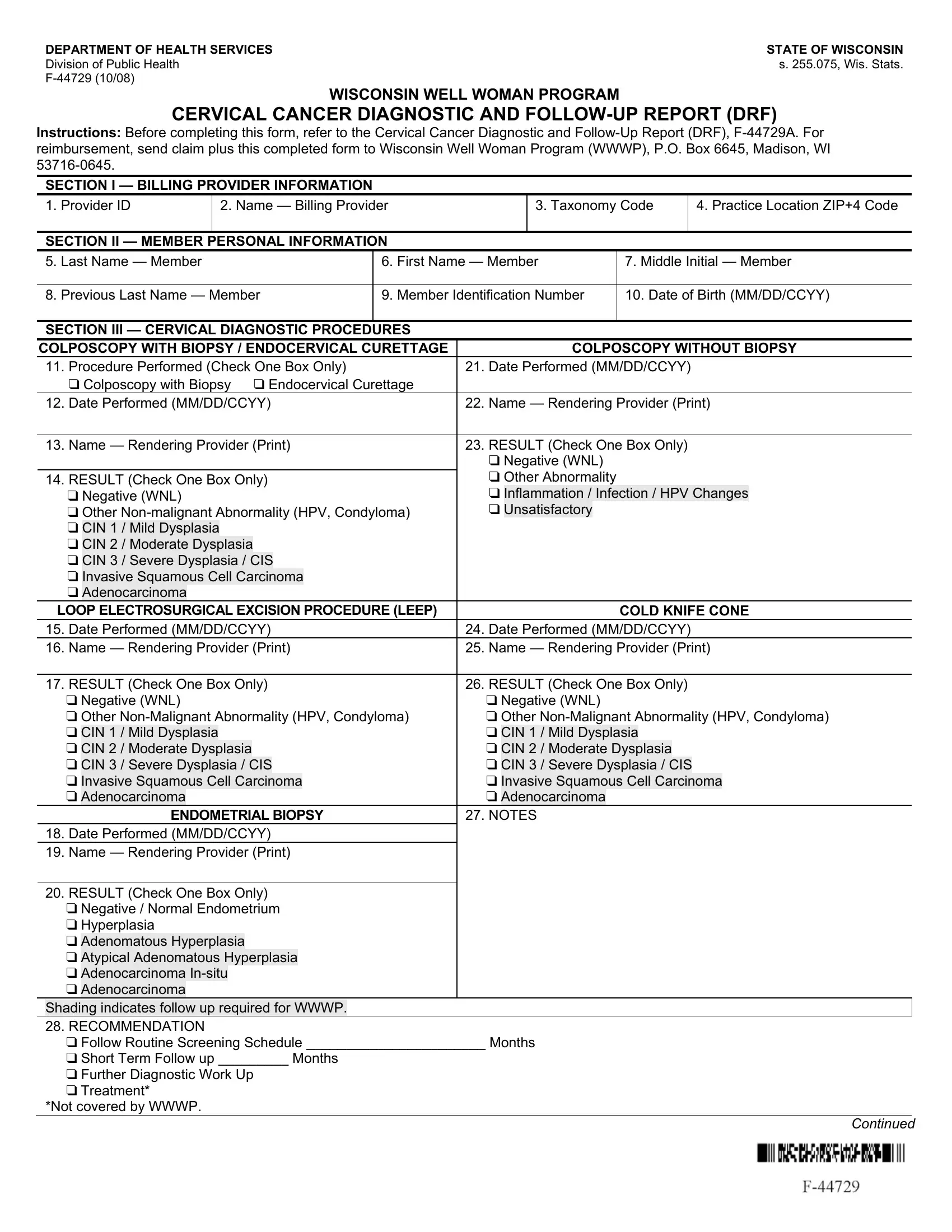
1. To start with, when completing the WNL, start out with the section that has the next blanks:
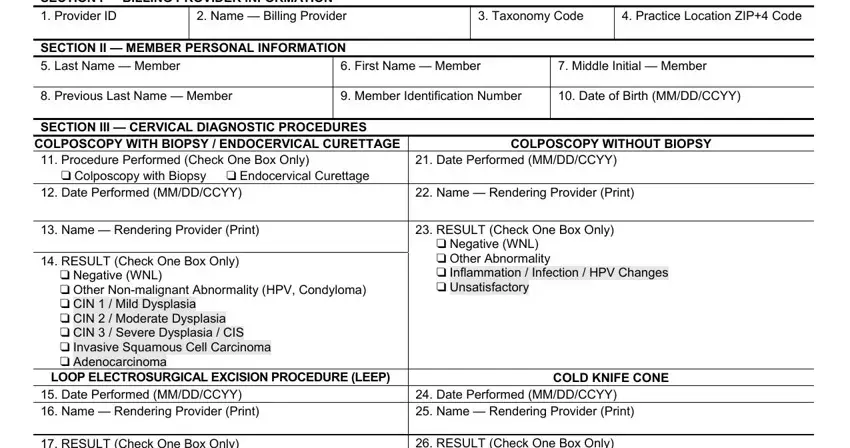
2. Now that this part is done, you'll want to include the necessary specifics in RESULT Check One Box Only cid, ENDOMETRIAL BIOPSY, Date Performed MMDDCCYY Name, RESULT Check One Box Only cid, and RESULT Check One Box Only cid so that you can progress further.
It's very easy to make an error when completing your RESULT Check One Box Only cid, so you'll want to look again prior to when you submit it.
3. Completing RESULT Check One Box Only cid, and Continued is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!

4. All set to begin working on this fourth portion! Here you have these cid Pending, cid Member Deceased, cid CIN Severe Dysplasia CIS, SECTION III CERVICAL DIAGNOSTIC, cid Stage II, cid Lost to Follow up, cid Refused Workup, cid CIN I Mild Dysplasia cid, Complete Treatment Date Treatment, cid Stage III, and cid Stage IV blanks to complete.

Step 3: Immediately after proofreading your entries, press "Done" and you are done and dusted! Join FormsPal right now and easily use WNL, ready for download. All alterations made by you are saved , which enables you to edit the form further as required. Here at FormsPal, we endeavor to be certain that all of your information is kept private.