In the realm of health services within the state of Wisconsin, the management and regulation of nurse aide training programs are critical components ensuring the highest standards of care and compliance with both state and federal regulations. The F-62224 form, as established by the Department of Health Services Division of Quality Assurance, plays a pivotal role in this regulatory framework. Specifically designed to notify the Division of Quality Assurance (DQA) about any substantial changes in approved nurse aide training programs, this document must be submitted at least 10 days before implementing any significant modifications. The term “substantial change” encompasses a wide range of adjustments, including alterations in the program's primary instructor, curriculum, classroom location, or clinical site. The importance of this form cannot be overstated, as failure to report such changes appropriately may lead to actions against the program, such as suspension, revocation of certification, or the requirement to implement a correction plan, in accordance with HFS 129, Wis. Admin. Code. The prescribed form, which must be completed in black ink or typed, seeks detailed information about the nature of the changes and mandates the inclusion of specific documentation concerning new personnel or program locations. By providing a structured process for reporting, the form ensures that all nurse aide training programs remain in compliance with the established regulations, thus upholding the integrity and quality of care provided by nurse aides in the state. Furthermore, the clear process for submission and the DQA's commitment to respond to all notices in writing reinforces the system's transparency and accountability.
| Question | Answer |
|---|---|
| Form Name | Form F 62224 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | F62224 wisconsin division of health notice of substantial change form |
DEPARTMENT OF HEALTH SERVICES |
STATE OF WISCONSIN |
|
Division of Quality Assurance |
42 |
CFR 483.75, Subpart D |
HFS |
129, Wis. Admin. Code |
|
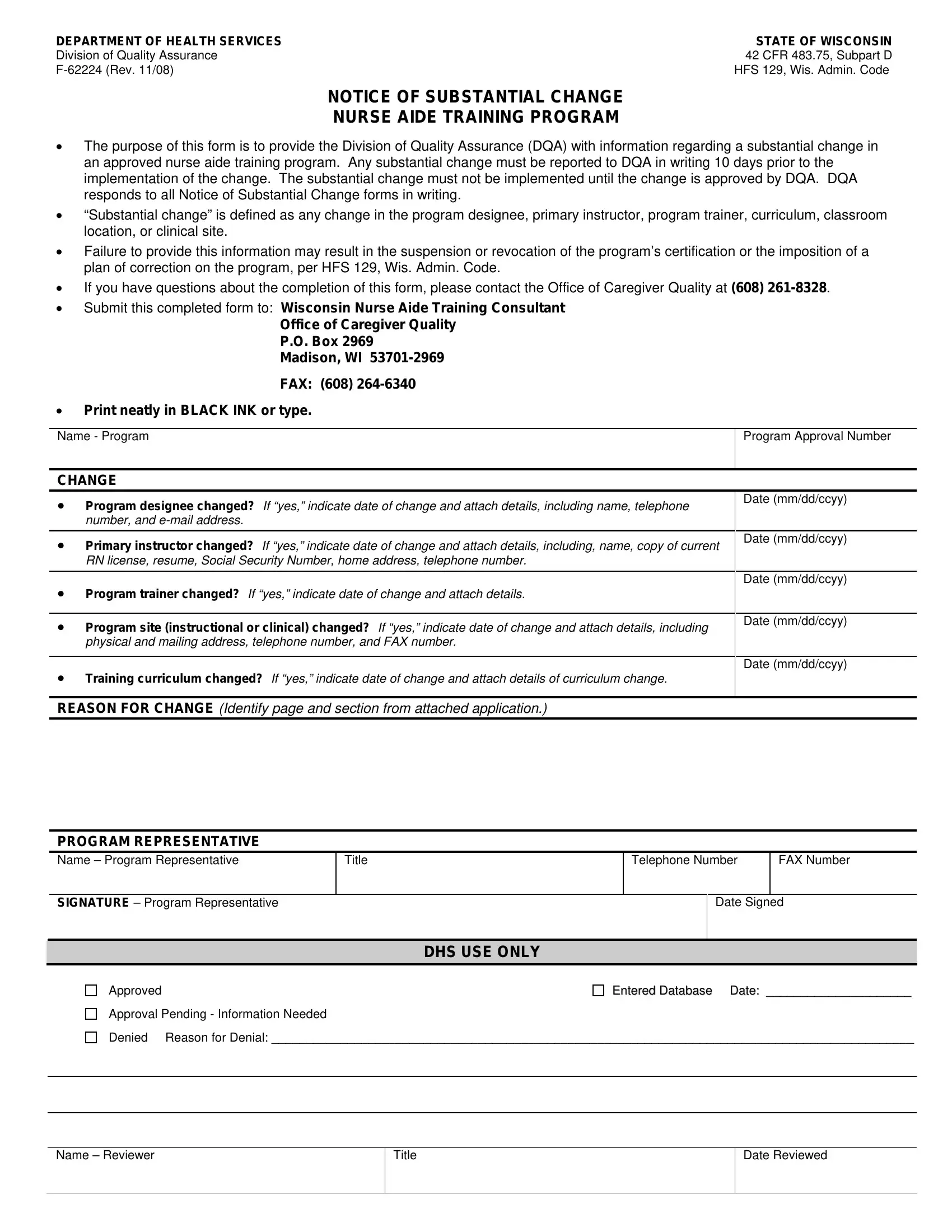
NOTICE OF SUBSTANTIAL CHANGE
NURSE AIDE TRAINING PROGRAM
•The purpose of this form is to provide the Division of Quality Assurance (DQA) with information regarding a substantial change in an approved nurse aide training program. Any substantial change must be reported to DQA in writing 10 days prior to the implementation of the change. The substantial change must not be implemented until the change is approved by DQA. DQA responds to all Notice of Substantial Change forms in writing.
•“Substantial change” is defined as any change in the program designee, primary instructor, program trainer, curriculum, classroom location, or clinical site.
•Failure to provide this information may result in the suspension or revocation of the program’s certification or the imposition of a plan of correction on the program, per HFS 129, Wis. Admin. Code.
•If you have questions about the completion of this form, please contact the Office of Caregiver Quality at (608)
•Submit this completed form to: Wisconsin Nurse Aide Training Consultant
Office of Caregiver Quality
P.O. Box 2969
Madison, WI
FAX: (608)
•Print neatly in BLACK INK or type.
Name - Program |
Program Approval Number |
|
|
CHANGE
• |
Program designee changed? If “yes,” indicate date of change and attach details, including name, telephone |
Date (mm/dd/ccyy) |
|
||
|
number, and |
|
|
|
|
• |
Primary instructor changed? If “yes,” indicate date of change and attach details, including, name, copy of current |
Date (mm/dd/ccyy) |
|
||
|
RN license, resume, Social Security Number, home address, telephone number. |
|
|
|
|
• |
|
Date (mm/dd/ccyy) |
Program trainer changed? If “yes,” indicate date of change and attach details. |
|
|
|
|
|
• |
Program site (instructional or clinical) changed? If “yes,” indicate date of change and attach details, including |
Date (mm/dd/ccyy) |
|
||
|
physical and mailing address, telephone number, and FAX number. |
|
|
|
|
• |
|
Date (mm/dd/ccyy) |
Training curriculum changed? If “yes,” indicate date of change and attach details of curriculum change. |
|
|
|
|
|
REASON FOR CHANGE (Identify page and section from attached application.)
PROGRAM REPRESENTATIVE
Name – Program Representative
Title
Telephone Number
FAX Number
SIGNATURE – Program Representative
Date Signed
|
DHS USE ONLY |
Approved |
Entered Database Date: _____________________ |
Approval Pending - Information Needed |
|
Denied |
Reason for Denial: _____________________________________________________________________________________________ |
|
|
|
|
Name – Reviewer
Title
Date Reviewed