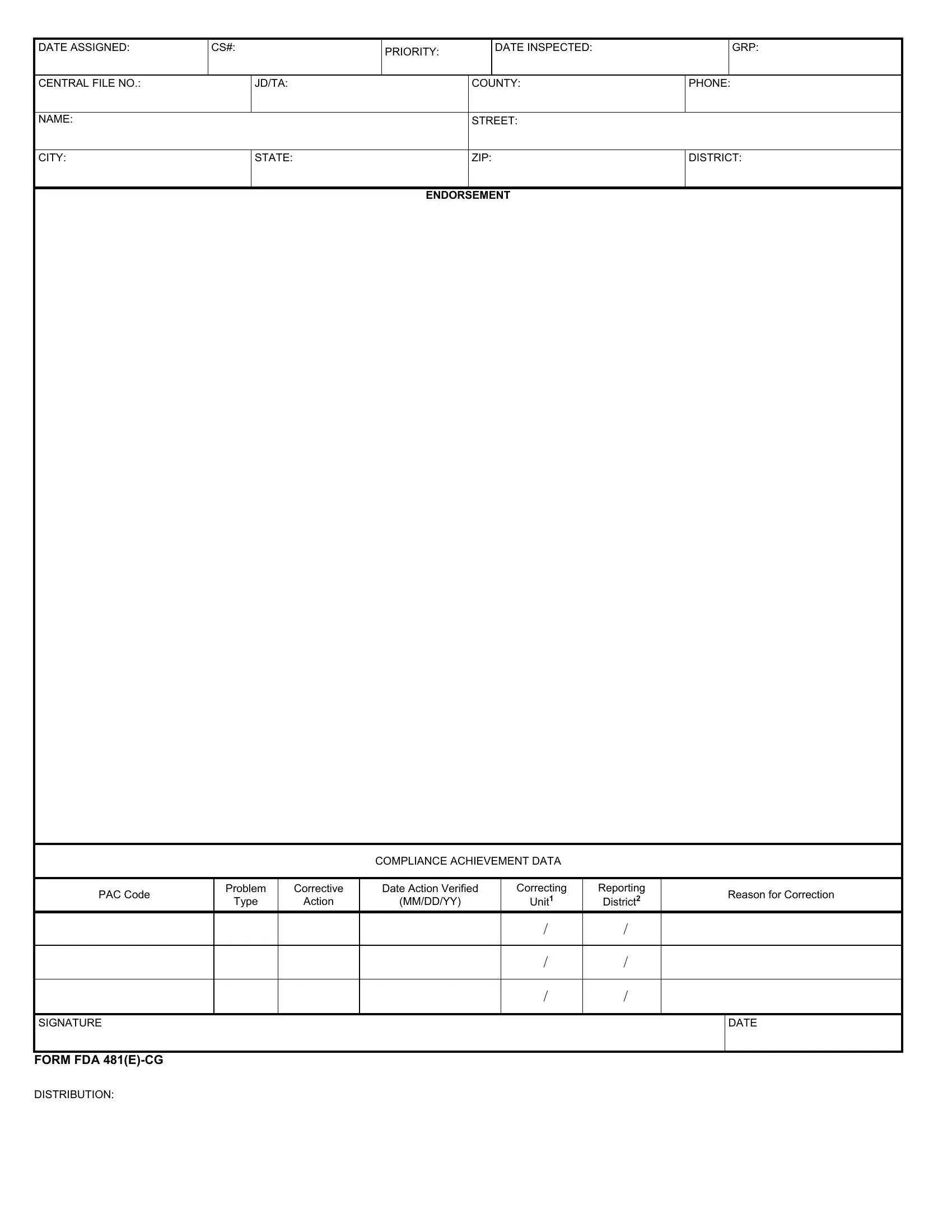
In the complex and regulatory-intensive landscape of healthcare and food safety, the FDA 481 form serves as a critical tool for ensuring compliance and quality across industries. Used by inspectors, this form captures a myriad of details pertaining to inspections conducted by the Food and Drug Administration (FDA). From basic establishment information, such as name, location, and contact details, to more intricate data including inspection dates, priority levels, and compliance outcomes, the form is exhaustive in scope. It also includes sections that detail the types of establishments inspected, reasons for inspections, corrective actions taken by firms, and verification of those actions. The FDA 481 form is instrumental in tracking compliance achievements and identifying areas requiring corrective measures, acting as a bridge between regulatory oversight and industry practices. By accommodating various segments like the date products covered, establishment changes, and samples collected, it aids in maintaining high standards of public health and safety. Furthermore, the inclusion of detailed endorsements, like compliance achievement data and the issuance of FDA Form 483 when violations are observed, underscores the form's role in fostering accountability and continuous improvement within regulated industries.
| Question | Answer |
|---|---|
| Form Name | Form FDA-481 |
| Form Length | 4 pages |
| Fillable? | Yes |
| Fillable fields | 439 |
| Avg. time to fill out | 29 min 37 sec |
| Other names | fda form 481, usfda forms 481, usfda forms 481 form, forms 481 |
DATE ASSIGNED: |
CS#: |
PRIORITY: |
|
DATE INSPECTED: |
|
GRP: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CENTRAL FILE NO.: |
|
JD/TA: |
|
COUNTY: |
PHONE: |
||
|
|
|
|
|
|
|
|
NAME: |
|
|
|
STREET: |
|
|
|
|
|
|
|
|
|
||
CITY: |
|
STATE: |
|
ZIP: |
DISTRICT: |
||
|
|
|
|
|
|
|
|
|
|
|
ENDORSEMENT |
|
|
||
COMPLIANCE ACHIEVEMENT DATA
PAC Code |
Problem |
Corrective |
Date Action Verified |
Correcting |
Reporting |
|
Reason for Correction |
Type |
Action |
(MM/DD/YY) |
Unit1 |
District2 |
|
||
|
|
|
|||||
|
|
|
|
/ |
/ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
/ |
/ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
/ |
/ |
|
|
|
|
|
|
|
|
|
|
SIGNATURE |
|
|
|
|
|
|
DATE |
|
|
|
|
|
|
|
|
FORM FDA |
|
|
|
|
|
|
|
DISTRIBUTION: |
|
|
|
|
|
|
|
DATE ASSIGNED: |
|
|
|
CS#: |
|
|
|
|
|
PRIORITY: |
|
|
DATE INSPD: |
|
|
|
GRP: |
|
|
|
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
CENTRAL FILE NO.: |
|
|
|
|
|
JD/TA: |
|
|
|
|
|
|
|
|
|
|
COUNTY: |
|
|
|
|
|
|
PHONE: |
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
NAME: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
STREET: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
CITY: |
|
|
|
|
|
|
|
STATE: |
|
|
|
|
|
|
|
|
|
|
ZIP: |
|
|
|
|
|
|
DISTRICT: |
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
RELATED FIRMS: |
|
|
|
|
|
|
|
|
STATE ASSIGNED: |
|
|
|
|
|
|
ITS: |
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
REGISTRATION: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
REG TYP |
|
MM/YY |
|
MM/YY |
|
|
MM/YY |
REG TYPE |
|
|
MM/YY |
|
|
MM/YY |
|
MM/YY |
|
REG TYPE |
|
MM/YY |
|
MMYY |
|
MM/YY |
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
F |
|
|
|
|
|
|
|
|
|
|
|
|
|
D |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
V |
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M |
|
|
|
|
|
|
|
|
|
|
|
|
|
R |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
B |
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1. |
|
|
|
|
|
|
|
|
|
|
|
2. |
|
|
|
|
|
|
|
|
|
3. |
|
|
|
|
|
|
|
|
|
ESTABLISHMENT TYPES/ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
INDUSTRY CODES ON OEI: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
TOTAL ESTAB |
|
|
|
INTERSTATE BUSINESS |
|
|
|
DISTRICT USE |
RECALL NUMBER |
|
REFUSAL CODE |
|
PROFILE |
|
PASS/FAIL |
|||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
SIZE |
|
|
RECEIVED |
SOLD |
|
|
|
#1 |
|
#2 |
#3 |
|
|
|
||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
ESTABLISHMENT CHANGES: |
New Firm |
None |
|
Name |
|
|
|
Address |
Ownership |
|
|
Size |
Prod Code |
|
Other |
Est Type |
||||||||||||||||||||||||
|
|
|
|
|
|
|
O/B |
Inactive |
|
Not OEI |
|
Aux Firm |
Registration |
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
Process |
|
|
|
|
|
|
|
Empl1 |
|
|
Empl2 |
|
|
Empl3 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
Est |
|
Insp |
|
PC: |
|
|
PC: |
|
|
PC: |
|
|
|
|
|
|
|
|
|
|
|
|
Resched |
Insp |
Dist |
||||||||||||
PAC |
|
(Product) |
|
|
|
|
|
|
|
|
|
|
|
Product |
|
|
Priority |
|||||||||||||||||||||||
|
|
Typ |
|
Basis |
|
No: |
|
|
No: |
|
|
No: |
|
|
|
|
|
|
|
Date |
Conc |
DSCN |
||||||||||||||||||
|
|
Code |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
HD: |
|
|
HD: |
|
|
HD: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
SAMPLES COLLECTED: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
SAMPLE #: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PRODUCT: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
HEADQUARTERS UNTI REFERRED: |
|
|
|
|
|
|
|
|
|
|
|
FDA 483 ISSUED: |
|
YES |
|
|
NO |
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
REASON REFERRED: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
OTHER FED GOVT INSP OR GRADING: |
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
INSPECTOR’S NAME AND SIGNATURE: |
|
|
|
|
|
|
|
|
|
|
|
SUPERVISOR’S NAME AND SIGNATURE: |
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
FORM FDA
DATE ASSIGNED: |
CS#: |
PRIORITY: |
|
DATE INSPD: |
|
GRP: |
|
|
|
|
|
|
|
|
|
CENTRAL FILE NO.: |
|
JD/TA: |
|
COUNTY: |
PHONE: |
||
|
|
|
|
|
|
|
|
NAME: |
|
|
|
STREET: |
|
|
|
|
|
|
|
|
|
||
CITY: |
|
STATE: |
|
ZIP: |
DISTRICT: |
||
|
|
|
|
|
|
|
|
PRODUCTS COVERED
DATE COVERED PRODUCT CODE EST TYPE EST TYP
EST TYP
PRODUCT DESCRIPTION
FORM FDA
DATE ASSIGNED: |
|
|
CS#: |
|
|
|
PRIORITY: |
|
DATE INSPECTED: |
|
|
|
GRP: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CENTRAL FILE NO.: |
|
|
|
JD/TA: |
|
|
|
COUNTY: |
|
PHONE: |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
NAME: |
|
|
|
|
|
|
|
STREET: |
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
||
CITY: |
|
|
|
STATE: |
|
|
|
ZIP: |
|
DISTRICT: |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
||
PROFILE DATA SHEET NO.: |
|
|
|
|
|
EMPLOYEE NUMBER: |
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PROFILE DATA SHEET |
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
||
PRO |
|
NEW STATUS |
CURRENT STATUS |
|
|
|
REMARKS |
|||||||
|
|
|
|
|
|
|
GMP DATE |
|
|
|||||
CLS |
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M |
|
R |
M |
R |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
||
SIGN OFF SIGNATURE |
|
|
|
|
|
|
|
|
|
|
DATE OF SIGNATURE |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
FORM FDA |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DISTRIBUTION: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|