

Dealing with PDF files online is actually a piece of cake with our PDF editor. Anyone can fill out Form Fm 16 here painlessly. To make our tool better and more convenient to utilize, we continuously come up with new features, taking into consideration feedback from our users. This is what you'll want to do to start:
Step 1: Open the PDF doc in our tool by clicking on the "Get Form Button" above on this page.
Step 2: With this handy PDF tool, it's possible to accomplish more than simply fill in blank fields. Edit away and make your documents seem professional with custom text added, or optimize the original input to excellence - all that comes along with an ability to incorporate your own photos and sign the file off.
This PDF doc will involve some specific details; to ensure correctness, you need to bear in mind the next tips:
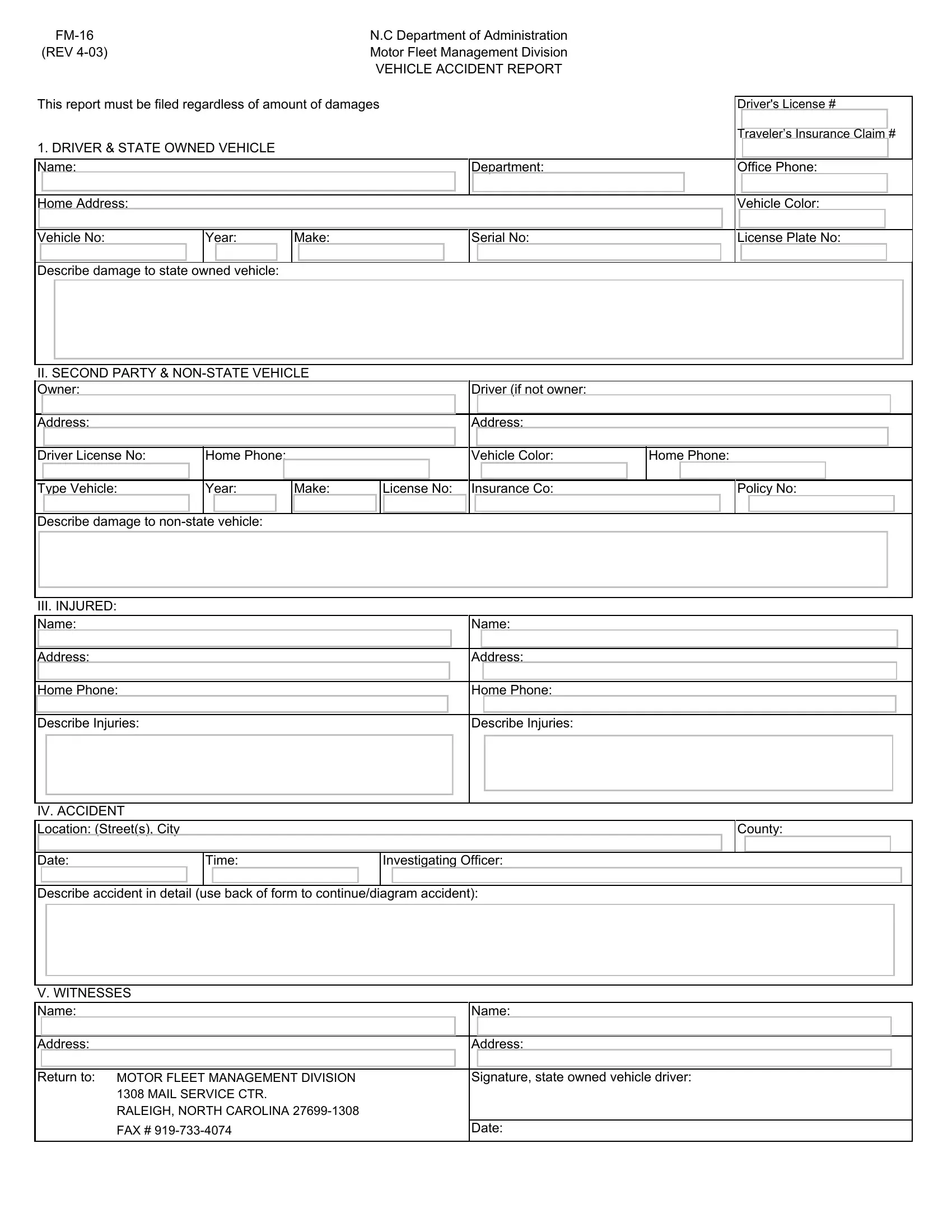
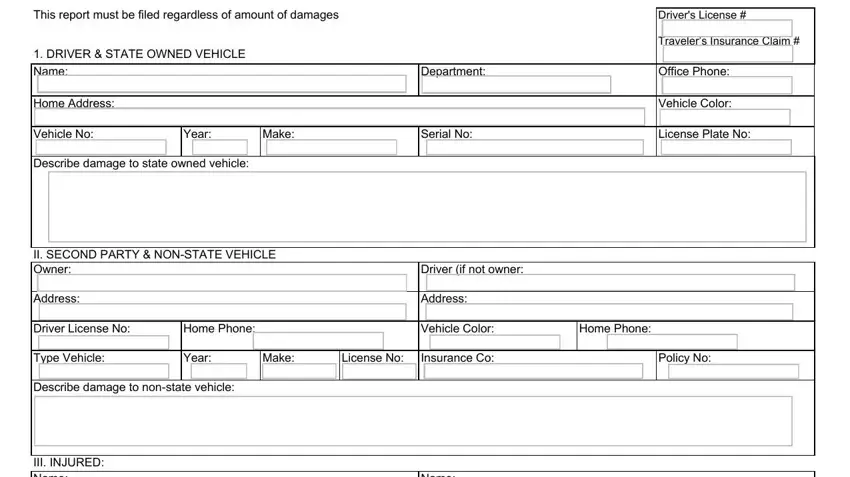
1. The Form Fm 16 will require particular information to be entered. Ensure that the next blanks are completed:
2. Immediately after this section is done, proceed to type in the suitable information in all these: III INJURED Name, Address, Home Phone Describe Injuries, IV ACCIDENT Location Streets City, Name, Address, Home Phone Describe Injuries, Date, Time, Investigating Officer, Describe accident in detail use, V WITNESSES Name, Address, Name, and Address.
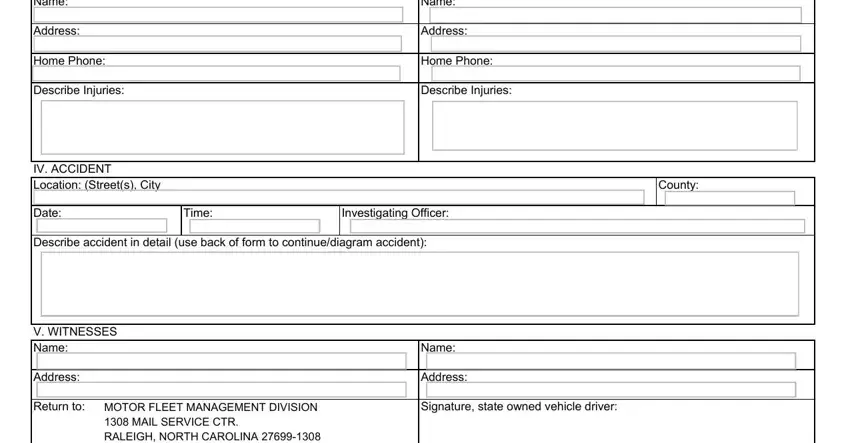
In terms of Time and Investigating Officer, ensure you get them right here. Those two are the most important ones in this page.
Step 3: Revise everything you've typed into the blanks and hit the "Done" button. Get your Form Fm 16 when you register here for a free trial. Immediately view the pdf in your personal account, along with any modifications and adjustments being all synced! FormsPal is devoted to the privacy of all our users; we make sure all information going through our editor remains secure.