
foh 6 from download can be filled in without any problem. Simply use FormsPal PDF editor to accomplish the job without delay. We are aimed at providing you the ideal experience with our editor by regularly adding new capabilities and enhancements. Our tool is now much more intuitive as the result of the latest updates! At this point, editing PDF forms is easier and faster than ever. If you are seeking to get started, this is what you will need to do:
Step 1: Access the PDF in our editor by pressing the "Get Form Button" above on this page.
Step 2: Once you launch the PDF editor, there'll be the document made ready to be filled in. Aside from filling in various blanks, you may also do other sorts of actions with the file, namely adding your own text, modifying the original textual content, inserting images, putting your signature on the form, and more.
If you want to finalize this PDF form, be sure you enter the required details in every single area:
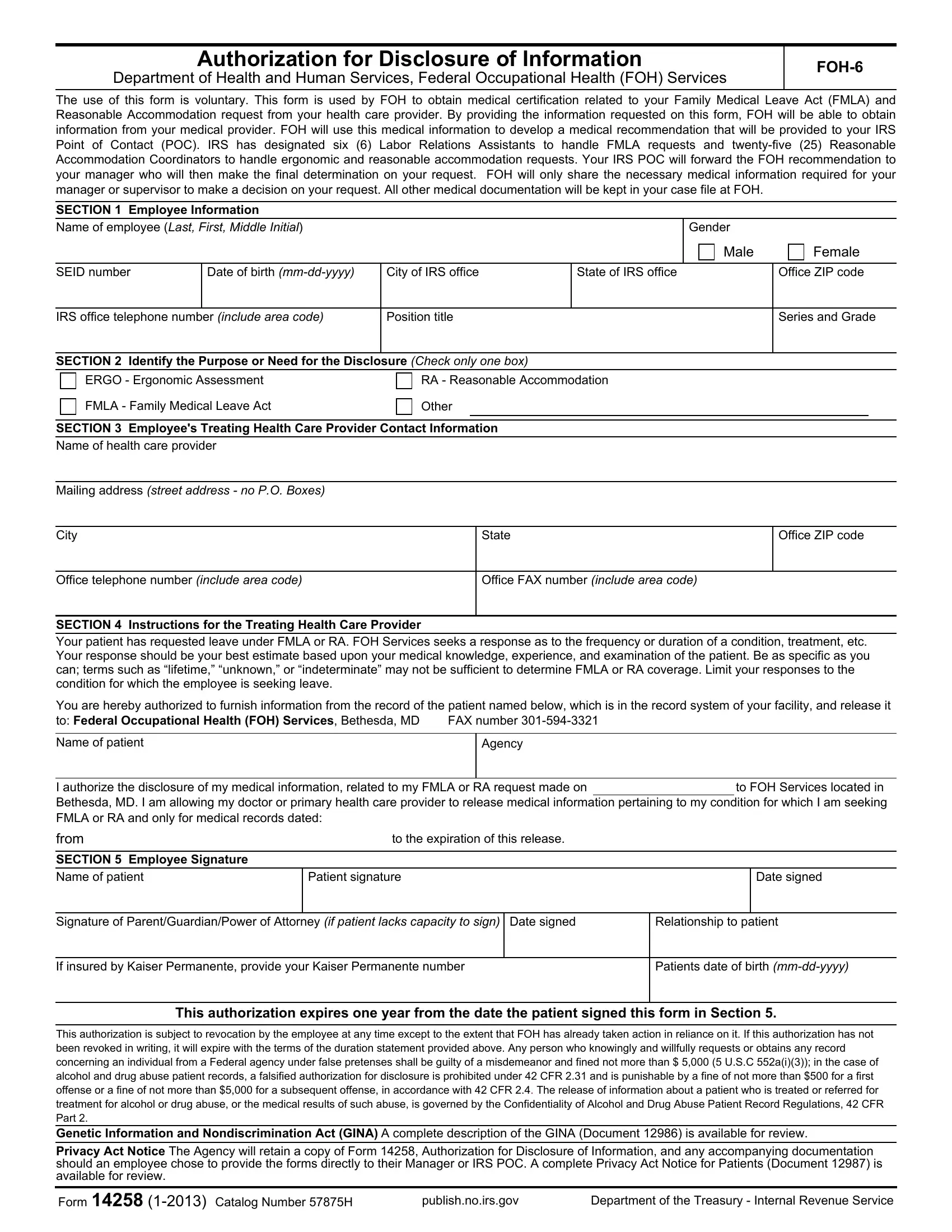
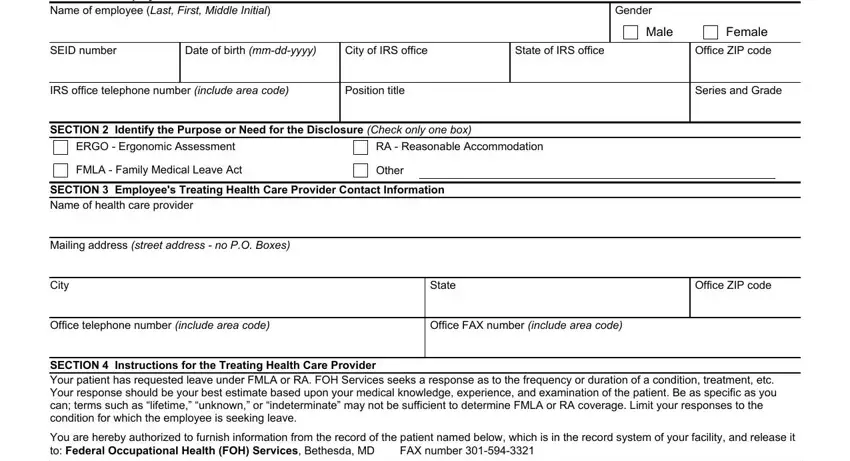
1. For starters, when filling out the foh 6 from download, begin with the form section that features the subsequent blank fields:
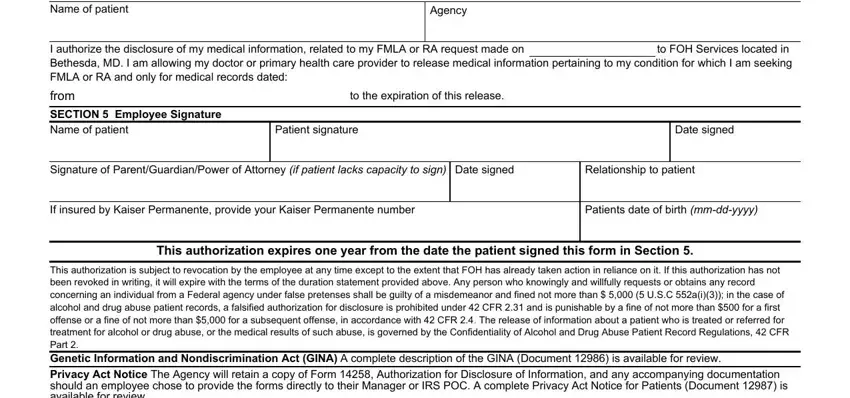
2. Soon after the first section is completed, go to enter the suitable details in all these: Name of patient, Agency, I authorize the disclosure of my, from, to the expiration of this release, SECTION Employee Signature Name, Patient signature, Date signed, Signature of ParentGuardianPower, Relationship to patient, If insured by Kaiser Permanente, Patients date of birth mmddyyyy, This authorization expires one, and This authorization is subject to.
Lots of people often make some errors while filling in Agency in this part. Don't forget to review whatever you type in right here.
Step 3: Right after you have looked over the details in the file's blank fields, just click "Done" to conclude your FormsPal process. Sign up with FormsPal now and easily use foh 6 from download, prepared for downloading. Each edit made is conveniently preserved , which means you can edit the document later as required. FormsPal is dedicated to the personal privacy of our users; we make sure that all personal data handled by our tool remains secure.