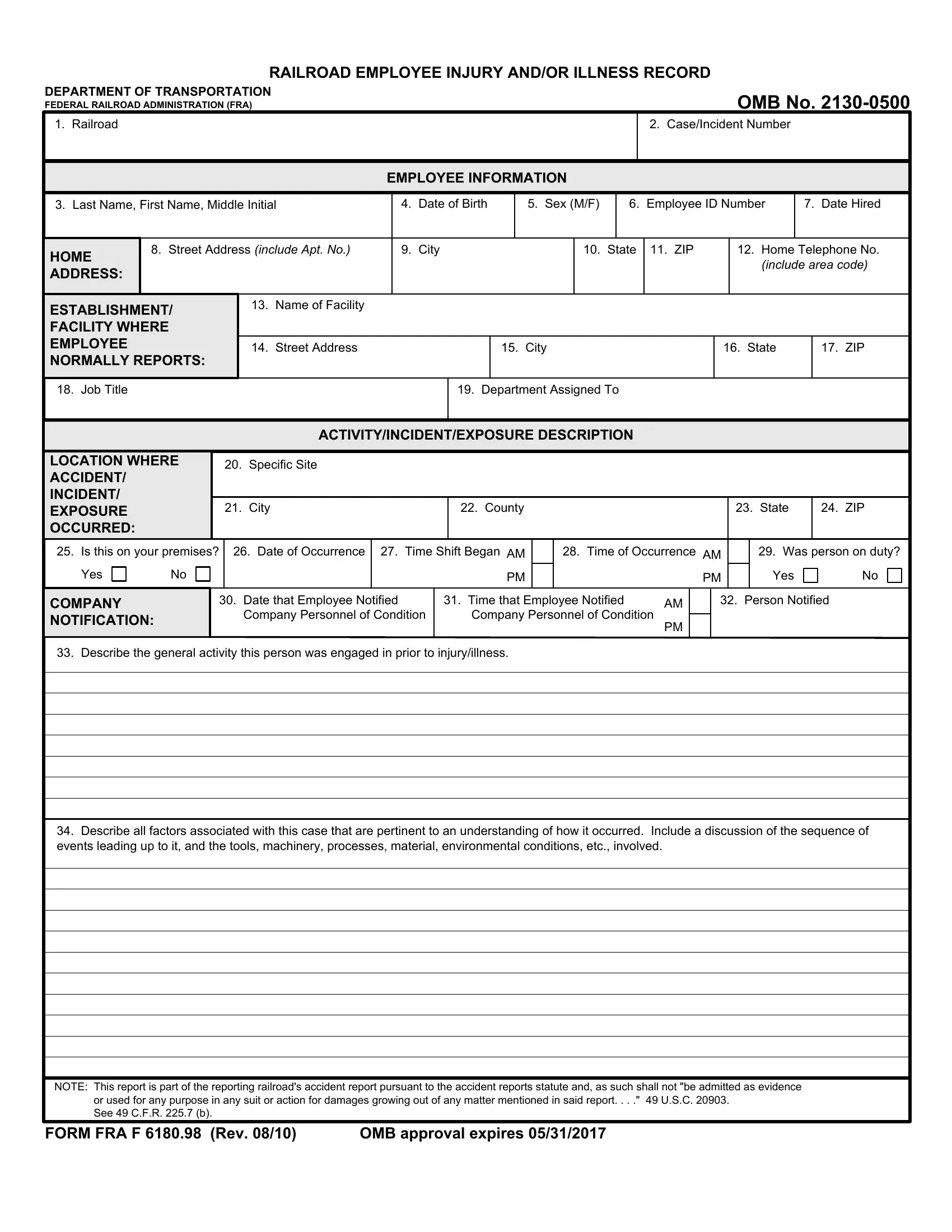
In the bustling world of the railroad industry, ensuring the safety and well-being of employees is paramount. This is where the Department of Transportation's Federal Railroad Administration (FRA) plays a crucial role, especially with the implementation of the FRA F 6180 98 form, officially known as the Railroad Employee Injury and/or Illness Record. This document is an essential tool for the meticulous reporting and tracking of any injuries or illnesses that occur among railroad workers. It meticulously gathers detailed information about the employee, including personal details, employment information, and the specifics of the incident, such as where, when, and how it happened. Additionally, it dives into the nature of the injury or illness, the treatment administered, and any significant consequences of the incident, such as death, hospitalization, or missed workdays. This form plays a critical role in maintaining safety standards within the railroad industry by facilitating a thorough investigation of accidents and exposures to hazardous conditions, with the ultimate goal of preventing future incidents. Moreover, it emphasizes the importance of transparency and accountability, requiring that the collected information be reported and made available as a matter of public record. By ensuring that every incident is properly documented and reported, the FRA F 6180 98 form contributes significantly to ongoing efforts to enhance rail safety across the nation.
| Question | Answer |
|---|---|
| Form Name | Form Fra F 6180 98 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | fra form 6180 97 fillable, fra f 98 download, fra f 6180 98, fra f 6180 56 |
RAILROAD EMPLOYEE INJURY AND/OR ILLNESS RECORD
DEPARTMENT OF TRANSPORTATION
FEDERAL RAILROAD ADMINISTRATION (FRA)
OMB No.
1. Railroad
2. Case/Incident Number
EMPLOYEE INFORMATION
|
3. Last Name, First Name, Middle Initial |
4. |
Date of Birth |
5. Sex (M/F) |
|
6. |
Employee ID Number |
7. Date Hired |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
HOME |
8. Street Address (include Apt. No.) |
9. |
City |
|
10. |
State |
11. ZIP |
12. Home Telephone No. |
||
|
|
|
|
|
|
|
|
|
(include area code) |
||
|
ADDRESS: |
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ESTABLISHMENT/ FACILITY WHERE EMPLOYEE NORMALLY REPORTS:
13. Name of Facility
14. Street Address |
15. City |
16. State |
17. ZIP |
|
|
|
|
18. Job Title |
19. Department Assigned To |
|
|
ACTIVITY/INCIDENT/EXPOSURE DESCRIPTION
LOCATION WHERE |
|
20. |
Specific Site |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
ACCIDENT/ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
INCIDENT/ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
EXPOSURE |
|
|
|
21. |
City |
|
22. County |
|
|
|
|
|
23. |
State |
24. |
ZIP |
||||||||||
OCCURRED: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
25. Is this on your premises? |
|
26. Date of Occurrence |
27. Time Shift Began AM |
|
28. Time of Occurrence AM |
|
|
29. Was person on duty? |
||||||||||||||||||
Yes |
|
|
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PM |
|
|
|
PM |
|
|
Yes |
|
|
|
No |
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
COMPANY |
|
|
|
30. |
Date that Employee Notified |
31. Time that Employee Notified |
AM |
|
32. Person Notified |
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
NOTIFICATION: |
|
|
|
|
|
Company Personnel of Condition |
|
Company Personnel of Condition |
PM |
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
33. Describe the general activity this person was engaged in prior to injury/illness.
34.Describe all factors associated with this case that are pertinent to an understanding of how it occurred. Include a discussion of the sequence of events leading up to it, and the tools, machinery, processes, material, environmental conditions, etc., involved.
NOTE: This report is part of the reporting railroad's accident report pursuant to the accident reports statute and, as such shall not "be admitted as evidence or used for any purpose in any suit or action for damages growing out of any matter mentioned in said report. . . ." 49 U.S.C. 20903.
See 49 C.F.R. 225.7 (b).
FORM FRA F 6180.98 (Rev. 08/10) |
OMB approval expires 05/31/2017 |
INJURY/CONDITION INFORMATION
35.Describe in detail the injury/condition that this person sustained. Include a discussion of the body parts affected. If this is a recurrence, list date of last occurrence.
36. Identify all persons and organizations used to evaluate and/or treat condition. (Include facility, provider, and address)
37. Describe all procedures, medications, therapy, etc., used/recommended for the treatment of condition:
38. Check any of the following consequences resulting from this injury/condition:
Death. Date of: _______________
Restriction of work. Reportable days of restricted activity: ____________ as of: ____________
Occupational illness. Date of initial diagnosis:
Instructions to obtain prescription medication, or receipt of prescription medication.
Hospitalization for treatment as an inpatient.
Multiple treatments or therapy sessions.
Loss of consciousness.
Missed a day of work or next shift. Reportable days absent from work: ____________ as of: ____________
Significant injury/illness, one meeting specific case criteria, or a covered data case.
Medical treatment. This includes any medical care or treatment beyond “first aid” that is given, or should have been given, regardless of who provided the treatment. “First Aid” treatment is limited to very simple procedures, e.g., application of a bandaid on minor scratches, cuts, abrasions, etc.
Transfer to another job or termination of employment.
39. If any of the above consequences occurred, the injury/condition is almost always reportable to FRA on Form FRA F 6180.55a. If you believe this case
does not meet the reporting criteria, you must give a brief explanation below of the basis for this decision. Was the case reported? |
Yes |
|
No |
|
40. |
Has this employee been provided an opportunity to review his or her file? |
Yes |
|
|
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
41. |
Preparer’s Name |
42. Preparer’s Title |
|
|
|
43. Telephone Number |
44. Date initially |
||
|
|
|
|
|
|
|
|
|
signed/completed |
|
|
|
|
|
|
|
|
|
|
This collection of information is mandatory under 49 CFR 225, and is used by FRA to monitor national rail safety. Public reporting burden is estimated to average 1 hour per response, including the time for reviewing instructions, searching existing databases, gathering and maintaining the data needed, and completing and reviewing the collection of information. The information collected is a matter of public record, and no confidentiality is promised to any respondent. Please note that an agency may not conduct or sponsor, and a person is not required to respond to a collection of information unless it displays a currently valid OMB control number. The OMB control number for this collection is