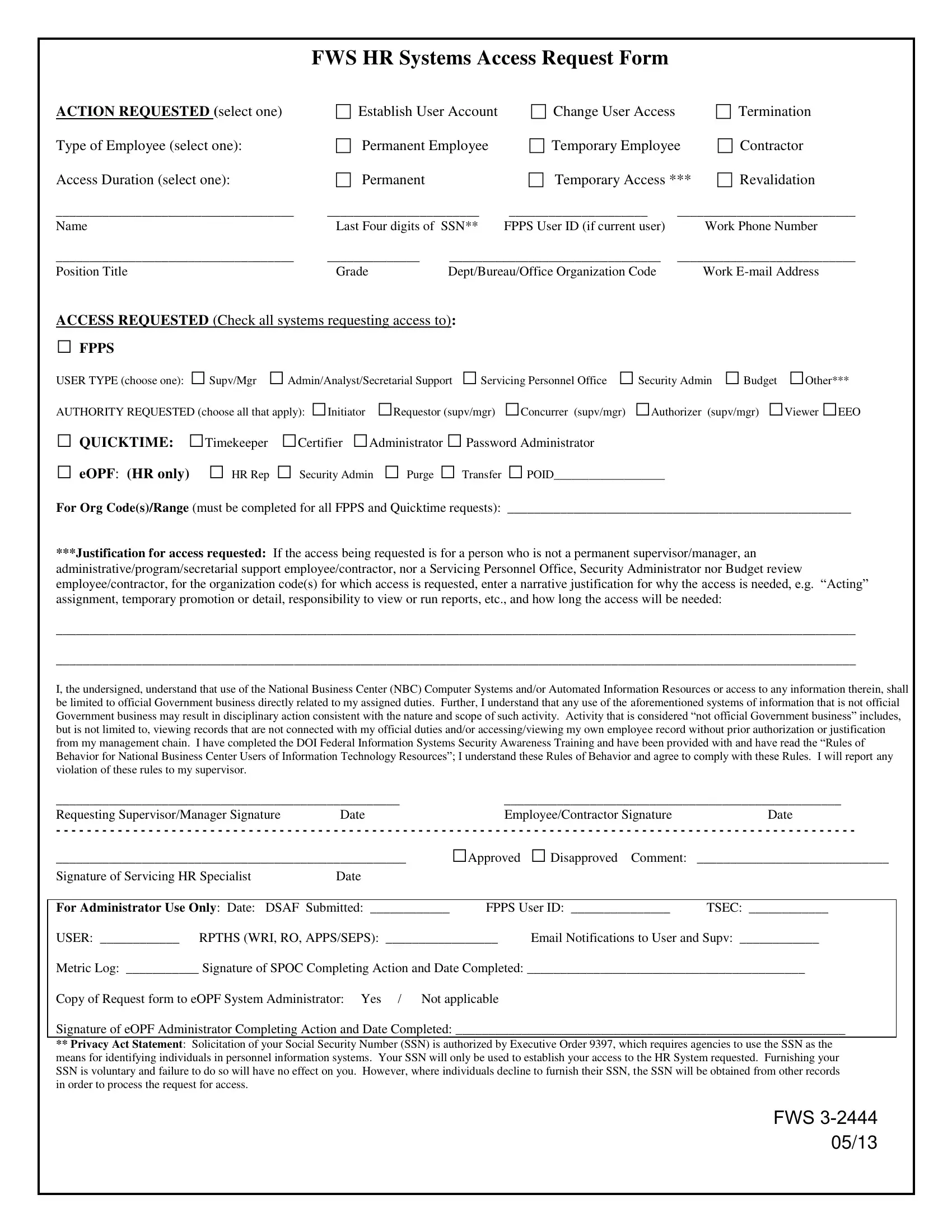
FWS HR Systems Access Request Form
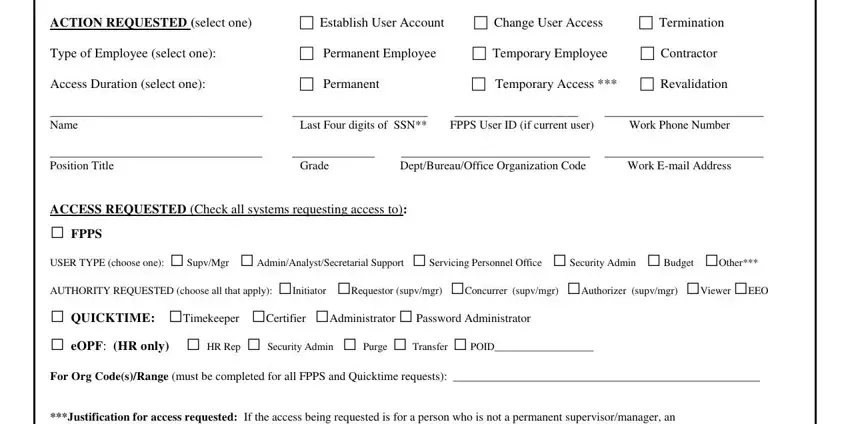
ACTION REQUESTED (select one) |
Establish User Account |
Change User Access |
|
Termination |
Type of Employee (select one): |
Permanent Employee |
Temporary Employee |
Contractor |
Access Duration (select one): |
Permanent |
|
Temporary Access *** |
Revalidation |
____________________________________ |
_______________________ |
_____________________ |
___________________________ |
Name |
Last Four digits of SSN** |
FPPS User ID (if current user) |
|
Work Phone Number |
____________________________________ |
______________ |
________________________________ |
___________________________ |
Position Title |
Grade |
Dept/Bureau/Office Organization Code |
|
Work E-mail Address |
ACCESS REQUESTED (Check all systems requesting access to):
□FPPS
USER TYPE (choose one): □ Supv/Mgr □ Admin/Analyst/Secretarial Support □ Servicing Personnel Office □ Security Admin □ Budget □Other***
AUTHORITY REQUESTED (choose all that apply): □Initiator □Requestor (supv/mgr) □Concurrer (supv/mgr) □Authorizer (supv/mgr) □Viewer □EEO
□ QUICKTIME: □Timekeeper □Certifier □Administrator □ Password Administrator
□eOPF: (HR only) □ HR Rep □ Security Admin □ Purge □ Transfer □ POID___________________
For Org Code(s)/Range (must be completed for all FPPS and Quicktime requests): ____________________________________________________
***Justification for access requested: If the access being requested is for a person who is not a permanent supervisor/manager, an
administrative/program/secretarial support employee/contractor, nor a Servicing Personnel Office, Security Administrator nor Budget review employee/contractor, for the organization code(s) for which access is requested, enter a narrative justification for why the access is needed, e.g. “Acting”
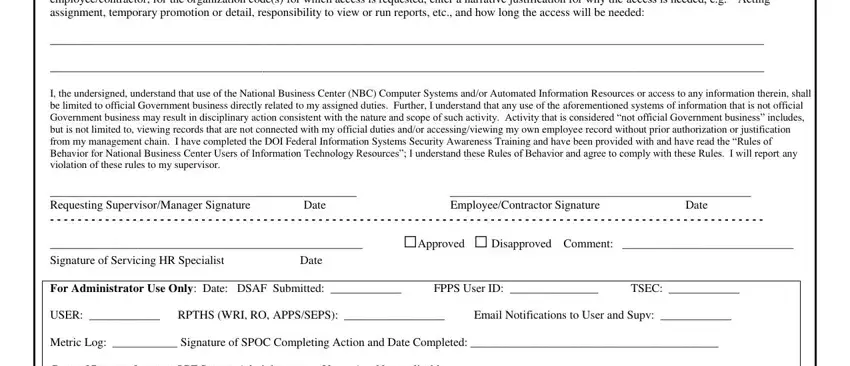
assignment, temporary promotion or detail, responsibility to view or run reports, etc., and how long the access will be needed:
_________________________________________________________________________________________________________________________
_________________________________________________________________________________________________________________________
I, the undersigned, understand that use of the National Business Center (NBC) Computer Systems and/or Automated Information Resources or access to any information therein, shall
be limited to official Government business directly related to my assigned duties. Further, I understand that any use of the aforementioned systems of information that is not official Government business may result in disciplinary action consistent with the nature and scope of such activity. Activity that is considered “not official Government business” includes,
but is not limited to, viewing records that are not connected with my official duties and/or accessing/viewing my own employee record without prior authorization or justification from my management chain. I have completed the DOI Federal Information Systems Security Awareness Training and have been provided with and have read the “Rules of Behavior for National Business Center Users of Information Technology Resources”; I understand these Rules of Behavior and agree to comply with these Rules. I will report any
violation of these rules to my supervisor.
____________________________________________________ |
___________________________________________________ |
Requesting Supervisor/Manager Signature |
Date |
Employee/Contractor Signature |
Date |
- - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - -
_____________________________________________________ |
□Approved |
□ Disapproved Comment: |
_____________________________ |
Signature of Servicing HR Specialist |
Date |
|
|
|
|
|
|
|
For Administrator Use Only: Date: |
DSAF Submitted: ____________ |
FPPS User ID: _______________ |
TSEC: ____________ |
USER: ____________ RPTHS (WRI, RO, APPS/SEPS): _________________ |
Email Notifications to User and Supv: ____________ |
Metric Log: ___________ Signature of SPOC Completing Action and Date Completed: __________________________________________
Copy of Request form to eOPF System Administrator: Yes / Not applicable
Signature of eOPF Administrator Completing Action and Date Completed: ___________________________________________________________
**Privacy Act Statement: Solicitation of your Social Security Number (SSN) is authorized by Executive Order 9397, which requires agencies to use the SSN as the means for identifying individuals in personnel information systems. Your SSN will only be used to establish your access to the HR System requested. Furnishing your SSN is voluntary and failure to do so will have no effect on you. However, where individuals decline to furnish their SSN, the SSN will be obtained from other records in order to process the request for access.
FWS 3-2444
05/13