
You are able to fill in medicaid 3038 form effectively with our online editor for PDFs. We at FormsPal are aimed at providing you the absolute best experience with our editor by constantly introducing new capabilities and enhancements. Our editor is now even more useful as the result of the latest updates! At this point, working with PDF documents is simpler and faster than ever before. For anyone who is seeking to get going, here's what it will take:
Step 1: Click on the "Get Form" button above on this webpage to open our PDF tool.
Step 2: This editor will let you change nearly all PDF forms in a range of ways. Enhance it by writing customized text, correct what's originally in the file, and include a signature - all at your convenience!
This form requires specific details to be typed in, hence you should take your time to provide precisely what is requested:
1. While submitting the medicaid 3038 form, be sure to incorporate all important blank fields within the associated area. This will help to facilitate the work, making it possible for your details to be handled without delay and correctly.
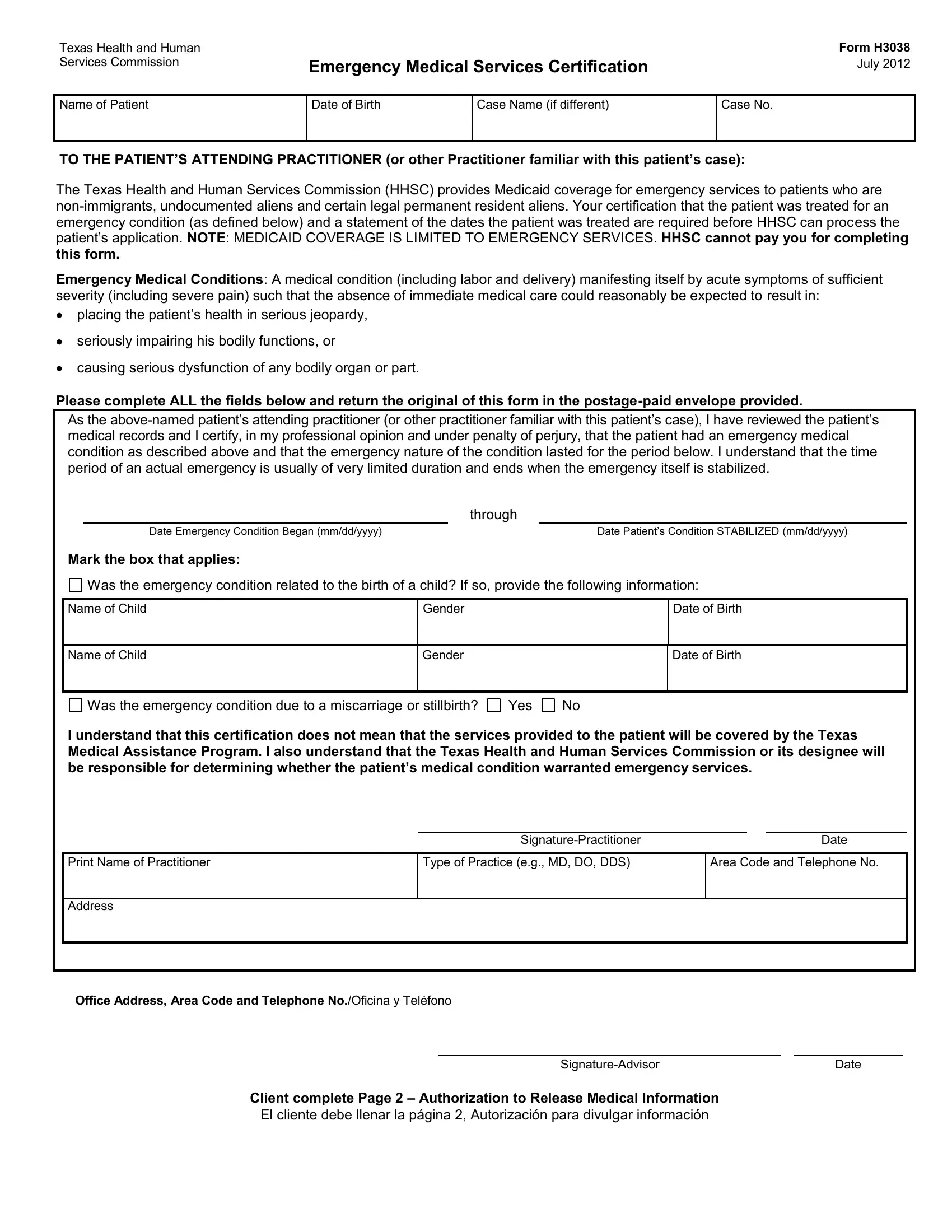
2. After filling in the last section, head on to the next stage and fill out the essential particulars in these blank fields - Name of Child, Name of Child, Gender, Gender, Date of Birth, Date of Birth, Was the emergency condition due to, Yes, I understand that this, SignaturePractitioner, Date, Print Name of Practitioner, Type of Practice eg MD DO DDS, Area Code and Telephone No, and Address.
3. Completing Office Address Area Code and, SignatureAdvisor, Date, Client complete Page, and El cliente debe llenar la página is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!
4. To go ahead, your next part involves completing a few blank fields. These comprise of SECTION ISECCIÓN I, Patients NameNombre del paciente, HHSC is requesting verification of, La HHSC necesita verificación de, I authorizeYo autorizo a, Doctor Medical Facilities or other, to complete Form H Emergency, This authorization expires onEsta, SECTION IISECCIÓN II, Client or Personal Representatives, Date Fecha, and If you are signing for the client, which are vital to going forward with this PDF.
5. This final stage to complete this PDF form is crucial. You'll want to fill out the required fields, and this includes Note If the person requesting the, SECTION IIISECCIÓN III, Notice to Client, Witness Testigo, Witness Testigo, HHSC as receiver of this, You can withdraw permission you, Date Fecha, Date Fecha, Aviso al cliente, La HHSC como destinatario de esta, and Usted puede retirar el permiso que, before submitting. Neglecting to do it could end up in an unfinished and possibly invalid paper!
Always be really attentive while filling in Note If the person requesting the and Witness Testigo, because this is where many people make a few mistakes.
Step 3: Look through what you've inserted in the blank fields and then click on the "Done" button. Go for a free trial subscription at FormsPal and acquire instant access to medicaid 3038 form - with all changes preserved and available inside your FormsPal account. FormsPal ensures your data confidentiality by having a protected method that in no way records or shares any kind of personal data provided. Rest assured knowing your files are kept protected each time you work with our editor!