Form HA-4608 |
(06-2021) UF |
Page 1 of 2 |
Social Security |
Administration |
OMB No. 0960-0284 |
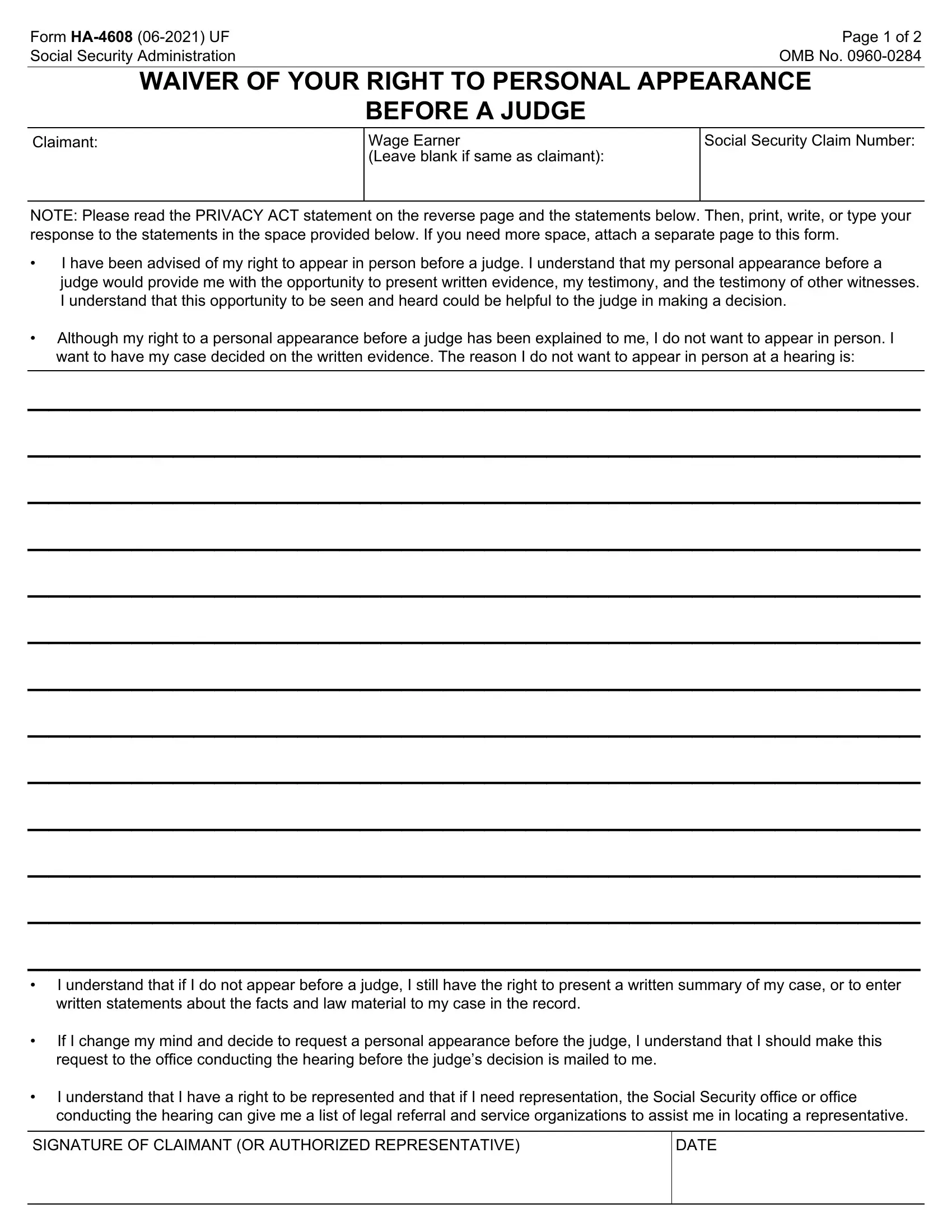
WAIVER OF YOUR RIGHT TO PERSONAL APPEARANCE
BEFORE A JUDGE
Wage Earner
(Leave blank if same as claimant):
Social Security Claim Number:
NOTE: Please read the PRIVACY ACT statement on the reverse page and the statements below. Then, print, write, or type your response to the statements in the space provided below. If you need more space, attach a separate page to this form.
•I have been advised of my right to appear in person before a judge. I understand that my personal appearance before a judge would provide me with the opportunity to present written evidence, my testimony, and the testimony of other witnesses. I understand that this opportunity to be seen and heard could be helpful to the judge in making a decision.
•Although my right to a personal appearance before a judge has been explained to me, I do not want to appear in person. I want to have my case decided on the written evidence. The reason I do not want to appear in person at a hearing is:
___________________________________________
___________________________________________
___________________________________________
___________________________________________
___________________________________________
___________________________________________
___________________________________________
___________________________________________
___________________________________________
___________________________________________
___________________________________________
___________________________________________
___________________________________________
•I understand that if I do not appear before a judge, I still have the right to present a written summary of my case, or to enter written statements about the facts and law material to my case in the record.
•If I change my mind and decide to request a personal appearance before the judge, I understand that I should make this request to the office conducting the hearing before the judge’s decision is mailed to me.
•I understand that I have a right to be represented and that if I need representation, the Social Security office or office conducting the hearing can give me a list of legal referral and service organizations to assist me in locating a representative.
SIGNATURE OF CLAIMANT (OR AUTHORIZED REPRESENTATIVE)
Form HA-4608 (06-2021) UF |
Page 2 of 2 |
|
|
Privacy Act Statement Collection and Use of Personal Information
Sections 205(a), 1631(e), and 1869(b) of the Social Security Act, as amended, allow us to collect this information. Furnishing us this information is voluntary. However, failing to provide all or part may prevent us from making an accurate and timely decision on your claim.
We will use the information you provide to continue processing the claim without an oral hearing. We may also share your information for the following purposes, called routine uses:
•To third party contacts in situations where the party to be contacted has, or is expected to have, information relating to the individual’s capability to manage his/her affairs or his/her eligibility for or entitlement to benefits under the Social Security program when the individual is unable to provide information being sought; or the data needed to establish the validity of evidence or to verify the accuracy of information presented by the individual; and
•To contractors and other Federal agencies, as necessary, for the purpose of assisting SSA in the efficient administration of its programs.
In addition, we may share this information in accordance with the Privacy Act and other Federal laws. For example, where authorized, we may use and disclose this information in computer matching programs, in which our records are compared with other records to establish or verify a person’s eligibility for Federal benefit programs and for repayment of incorrect or delinquent debts under these programs.
A list of additional routine uses is available in our Privacy Act System of Records Notices (SORN) 60-0009, entitled Hearing and Appeals Case Control System, as published in the Federal Register (FR) on October 13, 1982, at 47 FR 45589 and 60-0089, entitled Claims Folder System, as published in the FR on April 1, 2003, at 68 FR 15784. Additional information, and a full listing of all of our SORNs, is available on our website at www.ssa.gov/privacy/.
Paperwork Reduction Act Statement - This information collection meets the requirements of 44 U.S.C. § 3507, as amended by section 2 of the Paperwork Reduction Act of 1995. You do not need to answer these questions unless we display a valid Office of Management and Budget control number. We estimate that it will take about 2 minutes to read the instructions, gather the facts, and answer the questions. SEND OR BRING THE COMPLETED FORM TO YOUR LOCAL SOCIAL SECURITY OFFICE. You can find your local Social Security office through SSA’s website at www.socialsecurity.gov. Offices are also listed under
U. S. Government agencies in your telephone directory or you may call Social Security at 1-800-772-1213 (TTY
1-800-325-0778). You may send comments regarding this burden estimate or any other aspect of this collection, including suggestions for reducing this burden to: SSA, 6401 Security Blvd, Baltimore, MD 21235-6401. Send only comments relating to our time estimate or other aspects of this collection to this address, not the completed form.