Form Har 3 Connecticut is a serious, life-threatening condition that can affect anyone at any time. If you experience any of the symptoms associated with this condition, don't hesitate to seek medical help immediately. By understanding the causes and risk factors associated with Form Har 3 Connecticut, you can take steps to protect yourself and your loved ones. Stay informed and stay safe!
| Question | Answer |
|---|---|
| Form Name | Form Har 3 Connecticut |
| Form Length | 3 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 45 sec |
| Other names | HAR3_2011 ct health assessment form |
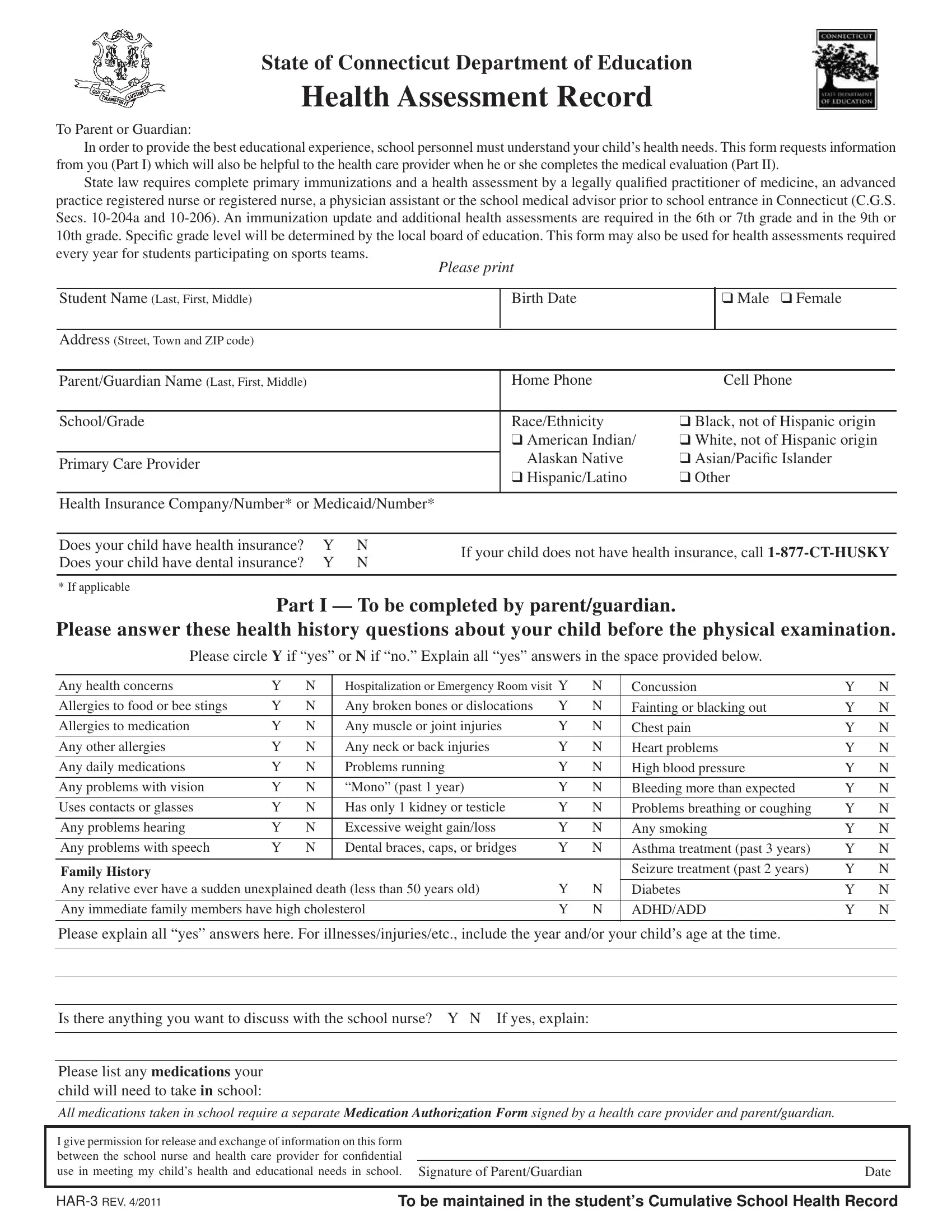
State of Connecticut Department of Education
Health Assessment Record
To Parent or Guardian:
In order to provide the best educational experience, school personnel must understand your child’s health needs. This form requests information from you (Part I) which will also be helpful to the health care provider when he or she completes the medical evaluation (Part II).
State law requires complete primary immunizations and a health assessment by a legally qualiied practitioner of medicine, an advanced
practice registered nurse or registered nurse, a physician assistant or the school medical advisor prior to school entrance in Connecticut (C.G.S.
Secs.
every year for students participating on sports teams.
Please print
Student Name (Last, First, Middle) |
Birth Date |
|
❑ Male ❑ Female |
|
|
|
|
|
|
Address (Street, Town and ZIP code) |
|
|
|
|
|
|
|
|
|
Parent/Guardian Name (Last, First, Middle) |
Home Phone |
|
Cell Phone |
|
|
|
|
||
School/Grade |
Race/Ethnicity |
❑ Black, not of Hispanic origin |
||
|
❑ American Indian/ |
❑ White, not of Hispanic origin |
||
|
Alaskan Native |
❑ Asian/Paciic Islander |
||
Primary Care Provider |
||||
|
❑ Hispanic/Latino |
❑ Other |
||
|
|
|
|
|
Health Insurance Company/Number* or Medicaid/Number*
Does your child have health insurance? |
Y |
N |
If your child does not have health insurance, call |
|
Does your child have dental insurance? |
Y |
N |
||
|
||||
|
|
|
|
|
* If applicable |
|
|
|
Part I — To be completed by parent/guardian.
Please answer these health history questions about your child before the physical examination.
Please circle Y if “yes” or N if “no.” Explain all “yes” answers in the space provided below.
Any health concerns |
Y |
N |
Hospitalization or Emergency Room visit Y |
N |
Concussion |
Y |
N |
|
Allergies to food or bee stings |
Y |
N |
Any broken bones or dislocations |
Y |
N |
Fainting or blacking out |
Y |
N |
Allergies to medication |
Y |
N |
Any muscle or joint injuries |
Y |
N |
Chest pain |
Y |
N |
Any other allergies |
Y |
N |
Any neck or back injuries |
Y |
N |
Heart problems |
Y |
N |
Any daily medications |
Y |
N |
Problems running |
Y |
N |
High blood pressure |
Y |
N |
Any problems with vision |
Y |
N |
“Mono” (past 1 year) |
Y |
N |
Bleeding more than expected |
Y |
N |
Uses contacts or glasses |
Y |
N |
Has only 1 kidney or testicle |
Y |
N |
Problems breathing or coughing |
Y |
N |
|
|
|
|
|
|
|
|
|
Any problems hearing |
Y |
N |
Excessive weight gain/loss |
Y |
N |
Any smoking |
Y |
N |
Any problems with speech |
Y |
N |
Dental braces, caps, or bridges |
Y |
N |
Asthma treatment (past 3 years) |
Y |
N |
|
|
|
|
|
|
|
|
|
Family History |
|
|
|
|
|
Seizure treatment (past 2 years) |
Y |
N |
Any relative ever have a sudden unexplained death (less than 50 years old) |
Y |
N |
Diabetes |
Y |
N |
|||
|
|
|
|
|
|
|||
Any immediate family members have high cholesterol |
Y |
N |
ADHD/ADD |
Y |
N |
|||
|
|
|
|
|
|
|
|
|
Please explain all “yes” answers here. For illnesses/injuries/etc., include the year and/or your child’s age at the time.
Is there anything you want to discuss with the school nurse? Y N If yes, explain:
Please list any medications your child will need to take in school:
All medications taken in school require a separate Medication Authorization Form signed by a health care provider and parent/guardian.
I give permission for release and exchange of information on this form between the school nurse and health care provider for conidential
use in meeting my child’s health and educational needs in school. Signature of Parent/Guardian |
Date |
|
|
|
|
TO BE MAINTAINED IN THE STUDENT’S CUMULATIVE SCHOOL HEALTH RECORD |
||
Part II — Medical Evaluation
Health Care Provider must complete and sign the medical evaluation and physical examination
Student Name |
|
Birth Date |
|
Date of Exam |
❑I have reviewed the health history information provided in Part I of this form
Physical Exam
Note: *Mandated Screening/Test to be completed by provider under Connecticut State Law
*Height _____ in. / _____% *Weight _____ lbs. / _____% |
BMI _____ / _____% Pulse _____ |
*Blood Pressure _____ / _____ |
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Normal |
|
Describe Abnormal |
|
|
Ortho |
|
|
Normal |
|
Describe Abnormal |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Neurologic |
|
|
|
|
|
|
Neck |
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
HEENT |
|
|
|
|
|
|
Shoulders |
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
*Gross Dental |
|
|
|
|
|
|
Arms/Hands |
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Lymphatic |
|
|
|
|
|
|
Hips |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Heart |
|
|
|
|
|
|
Knees |
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Lungs |
|
|
|
|
|
|
Feet/Ankles |
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Abdomen |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
*Postural |
❑ No spinal |
❑ Spine abnormality: |
|||||||||
|
|
|
|
|
|
|
|
||||||||||
Genitalia/ hernia |
|
|
|
|
|
|
|
|
abnormality |
|
❑ Mild |
❑ Moderate |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
❑ Marked ❑ Referral made |
|||
Skin |
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Screenings |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
*Vision Screening |
|
|
|
*Auditory Screening |
|
|
|
|
|
|
|
Date |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
Type: |
Right |
Left |
|
Type: |
Right |
Left |
|
|
Lead: |
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
❑ Pass |
❑ Pass |
|
|
|
|
|
|
||||
|
With glasses |
20/ |
20/ |
|
|
|
|
*HCT/HGB: |
|
|
|
||||||
|
|
|
|
|
|
|
❑ Fail |
❑ Fail |
|
|
|
|
|
|
|
|
|
|
Without glasses |
20/ |
20/ |
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
*Speech (school entry only) |
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
||||||||
|
❑ Referral made |
|
|
|
❑ Referral made |
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
Other: |
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
TB: |
❑ No |
❑ Yes |
|
PPD date read: |
|
|
Results: |
|
|
|
Treatment: |
|
|
|
||
*IMMUNIZATIONS
❑Up to Date or ❑
*Chronic Disease Assessment:
Asthma |
❑ No |
❑ Yes: |
❑ Intermittent ❑ Mild Persistent ❑ Moderate Persistent ❑ Severe Persistent ❑ Exercise induced |
||||
|
If yes, please provide a copy of the Asthma Action Plan to School |
|
|||||
Anaphylaxis ❑ No |
❑ Yes: |
❑ Food |
❑ Insects |
❑ Latex |
❑ Unknown source |
|
|
Allergies |
If yes, please provide a copy of the Emergency Allergy Plan to School |
|
|||||
|
History of Anaphylaxis |
❑ No |
❑ Yes |
Epi Pen required ❑ No |
❑ Yes |
||
Diabetes |
❑ No |
❑ Yes: |
❑ Type I |
❑ Type II |
Other Chronic Disease: |
|
|
Seizures |
❑ No |
❑ Yes, type: |
|
|
|
|
|
❑This student has a developmental, emotional, behavioral or psychiatric condition that may affect his or her educational experience. Explain: ____________________________________________________________________________________________________
Daily Medications (specify): ____________________________________________________________________________________
This student may: ❑ participate fully in the school program
❑participate in the school program with the following restriction/adaptation: _____________________________
___________________________________________________________________________________________________________
This student may: ❑ participate fully in athletic activities and competitive sports
❑participate in athletic activities and competitive sports with the following restriction/adaptation: ____________
___________________________________________________________________________________________________________
❑Yes ❑ No Based on this comprehensive health history and physical examination, this student has maintained his/her level of wellness.
Is this the student’s medical home? ❑ Yes ❑ No ❑ I would like to discuss information in this report with the school nurse.
|
|
|
|
|
|
Signature of health care provider MD / DO / APRN / PA |
Date Signed |
Printed/Stamped Provider Name and Phone Number |
|
|
|
|
|
|
Student Name: ______________________________________ Birth Date: ___________________
Immunization Record
To the Health Care Provider: Please complete and initial below.
Vaccine (Month/Day/Year) Note: *Minimum requirements prior to school enrollment. At subsequent exams, note booster shots only.
|
Dose 1 |
Dose 2 |
|
Dose 3 |
|
Dose 4 |
|
Dose 5 |
|
Dose 6 |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
DTP/DTaP |
* |
* |
|
* |
|
* |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DT/Td |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Tdap |
* |
|
|
|
|
|
|
Required for 7th grade entry |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
IPV/OPV |
* |
* |
|
* |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MMR |
* |
* |
|
|
|
|
|
Required |
||||
|
|
|
|
|
|
|
|
|
|
|
||
Measles |
* |
* |
|
|
|
|
|
Required |
||||
|
|
|
|
|
|
|
|
|
|
|
||
Mumps |
* |
* |
|
|
|
|
|
Required |
||||
|
|
|
|
|
|
|
|
|
|
|
||
Rubella |
* |
* |
|
|
|
|
|
Required |
||||
|
|
|
|
|
|
|
|
|
|
|
||
HIB |
* |
|
|
|
|
|
|
PK and K (Students under age 5) |
||||
|
|
|
|
|
|
|
|
|
|
|
||
Hep A |
* |
* |
|
|
|
|
|
PK and K (born 1/1/2007 or later) |
||||
|
|
|
|
|
|
|
|
|
|
|
||
Hep B |
* |
* |
|
* |
|
|
|
Required |
||||
|
|
|
|
|
|
|
|
|
|
|
||
Varicella |
* |
* |
|
|
|
|
|
2 doses required for K & 7th grade as of 8/1/2011 |
|
|||
|
|
|
|
|
|
|
|
|
|
|
||
PCV |
* |
|
|
|
|
|
|
PK and K (born 1/1/2007 or later) |
||||
|
|
|
|
|
|
|
|
|
|
|
||
Meningococcal |
* |
|
|
|
|
|
|
Required for 7th grade entry |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
HPV |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Flu |
* |
|
|
|
|
|
|
PK students |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
Other |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
Disease Hx ________________________________ |
________________________________ |
________________________________ |
|
|
||||||||
of above |
(Specify) |
|
|
(Date) |
|
|
|
(Conirmed by) |
|
|
|
|
|
|
|
|
Exemption |
|
|
|
|
|
|
|
|
|
Religious _____ Medical: Permanent _____ |
Temporary _____ Date _____ |
|
|
|
|||||||
|
Recertify Date _________ |
Recertify Date _________ Recertify Date ________ |
|
|
|
|||||||
Immunization Requirements for Newly Enrolled Students at Connecticut Schools
KINDERGARTEN
•DTaP: At least 4 doses. The last dose must be given on or after 4th birthday.
•Polio: At least 3 doses. The last dose must be given on or after 4th birthday.
•MMR: 2 doses given at least 28 day apart – 1st dose on or after the 1st birthday.
•Hib: 1 dose on or after 1st birthday (Children 5 years and older do not need proof of Hib vaccination).
•Pneumococcal: 1 dose on or after 1st birthday (born 1/1/2007 or later and less than 5 years old).
•Hep A: 2 doses given six months
•Hep B: 3
•Varicella: For students enrolled before August 1, 2011, 1 dose given on or after 1st birthday; for students enrolled on or after August 1, 2011
2 doses given 3 months apart – 1st dose on or after 1st birthday or veriication of disease*.
GRADES
•DTaP /Td/Tdap: At least 4 doses. The last dose must be given on or after 4th birthday;
students who start the series at age 7 or older only need a total of 3 doses of
•Polio: At least 3 doses. The last dose must be given on or after 4th birthday.
•MMR: 2 doses given at least 28 days apart- 1st dose on or after the 1st birthday.
•Hep B: 3 doses – the last dose on or after 24 weeks of age.
•Varicella: 1 dose on or after the 1st birthday or veriication of disease*.
GRADE 7
•Tdap/Td: 1 dose of Tdap for students 11 yrs. or older enrolled in 7th grade who completed their primary DTaP series; For those students who start the series at age 7 or older a total of 3 doses of
•Polio: At least 3 doses. The last dose must be given on or after 4th birthday.
•MMR: 2 doses given at least 28 days apart – 1st dose on or after the 1st birthday.
•Meningococcal: one dose for students enrolled in 7th grade.
•Hep B: 3
•Varicella: 2 doses given 3 months apart – 1st dose on or after 1st birthday or veriication of
disease*.
GRADES
•Td: At least 3 doses. Students who start the series at age 7 or older only need a total of 3 doses of
•Polio: At least 3 doses. The last dose must be given on or after 4th birthday.
•MMR: 2 doses given at least 28 days apart- 1st dose on or after the 1st birthday.
•Hep B: 3
•Varicella: For students <13 years of age, 1 dose given on or after the 1st birthday. For
students 13 years of age or older, 2 doses given at least 4 weeks apart or veriication of
disease*.
*Veriicationofdisease:Conirmation in writ- ing by a MD, PA, or APRN that the child has a previous history of disease, based on family or medical history.
|
|
|
|
|
|
Initial/Signature of health care provider MD / DO / APRN / PA |
Date Signed |
Printed/Stamped Provider Name and Phone Number |
|
|
|
|
|
|