
If you want to fill out Form Hca 50 224, you don't need to download any applications - simply try using our PDF editor. Our editor is continually evolving to provide the very best user experience attainable, and that's thanks to our resolve for continual improvement and listening closely to feedback from customers. Here is what you will need to do to begin:
Step 1: Press the "Get Form" button at the top of this page to get into our tool.
Step 2: With our advanced PDF editor, you can accomplish more than simply fill in forms. Try each of the functions and make your documents look sublime with customized textual content put in, or optimize the file's original content to excellence - all comes along with an ability to add almost any images and sign the PDF off.
Completing this form requires care for details. Make certain every blank is done properly.
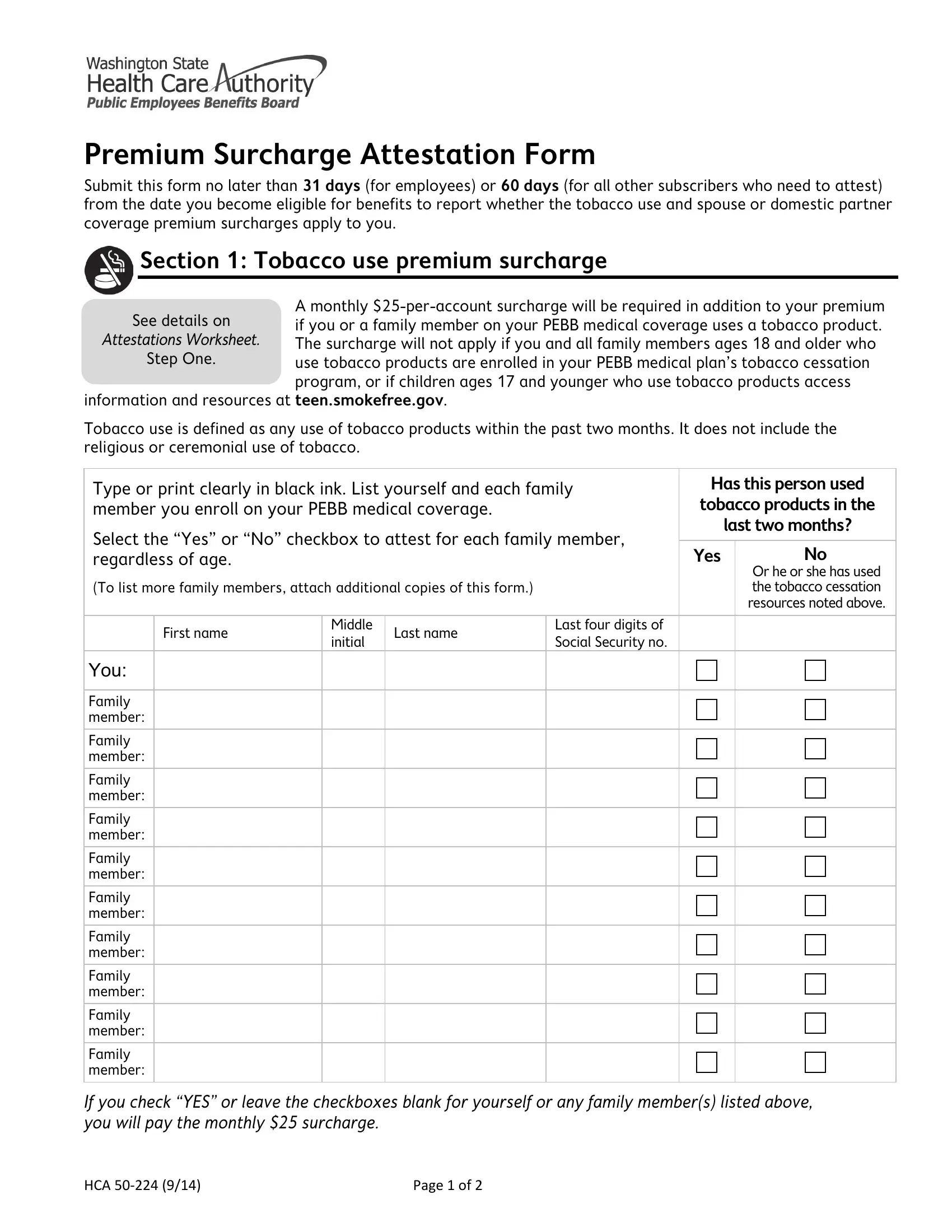
1. It's important to complete the Form Hca 50 224 accurately, therefore be mindful when filling out the areas containing these fields:
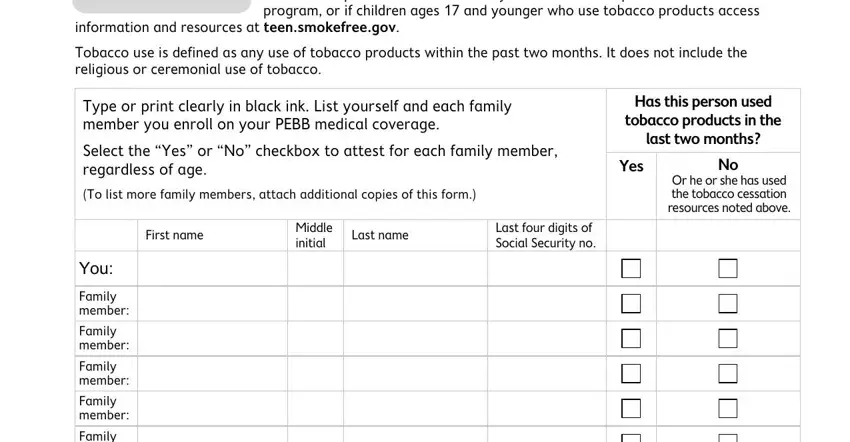
2. Soon after filling in this step, go to the next stage and enter the necessary particulars in these blanks - Family member, Family member, Family member, Family member, Family member, Family member, If you check YES or leave the, HCA, and Page of.
3. Completing Does the spouse or domestic, Yes, I used the Attestations Worksheet, Find the Spousal Plan Calculator, I used the Attestations Worksheet, Employer or PEBB Program to, I used the Attestations Worksheet, If you enroll a spouse or domestic, Section Signature, and By signing this form I declare is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!
As to I used the Attestations Worksheet and I used the Attestations Worksheet, make certain you get them right here. The two of these are the most significant ones in this PDF.
4. All set to fill out this fourth section! Here you'll get all these HCAs Privacy Notice We will keep, Name print Last four digits of, Signature Date, Agency name employees only, Please sign and date this form, If youre, An employee, Any other subscriber, Return it to, Your personnel payroll or benefits, PEBB Program Washington State, and Attach your printed Spousal Plan form blanks to fill in.
Step 3: Soon after rereading the fields, hit "Done" and you're all set! Get hold of your Form Hca 50 224 when you register at FormsPal for a 7-day free trial. Quickly view the pdf file in your FormsPal cabinet, together with any modifications and adjustments being all kept! FormsPal is invested in the personal privacy of our users; we make certain that all personal information entered into our tool stays confidential.