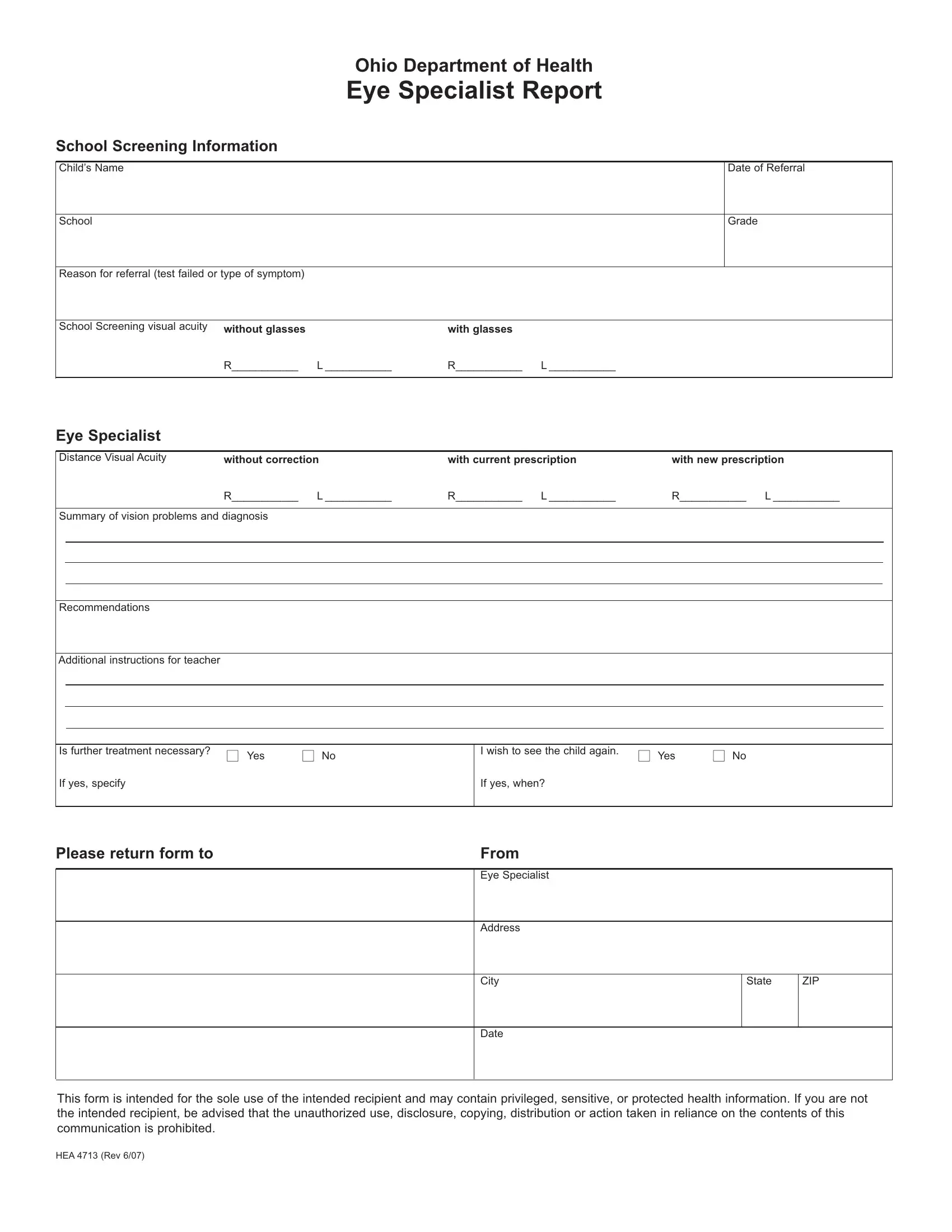
The HEA 4713 form, issued by the Ohio Department of Health, plays a crucial role in the health and academic performance of children by bridging the gap between school-based vision screenings and professional eye care. This detailed document captures a wide range of information, beginning with basic student identification details such as the child's name, date of referral, school, and grade, which sets the foundation for a comprehensive account of the child's visual health. It specifies the reason for referral, which could be a failed test or a particular symptom, and includes screening results both with and without glasses, offering a preliminary sense of the child's visual acuity. More in-depth analysis comes from the eye specialist's report, which assesses distance visual acuity across three conditions: without correction, with the current prescription, and with a new prescription, offering a nuanced view of the child's vision and any improvements with corrective measures. Furthermore, the form provides a summary of vision problems and diagnosis, alongside recommendations and additional instructions for teachers, which highlights any further treatment required and whether the child needs to be seen again. This document underscores the importance of early and accurate identification of vision issues, facilitating appropriate interventions that can significantly impact a child’s learning and overall quality of life. With spaces for the eye specialist's details and a note on the confidentiality of the information contained, the HEA 4713 form is a pivotal tool in promoting child health and educational success, embodying a meticulous approach to linking clinical findings with practical recommendations for school environments.
| Question | Answer |
|---|---|
| Form Name | Form Hea 4713 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | disclosure, Referral, eye doctor prescription template, glasses prescription form pdf |
|
|
|
Ohio Department of Health |
|
|
|
|
|
|||
|
|
|
Eye Specialist Report |
|
|
|
|
|
|||
School Screening Information |
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
Child’s Name |
|
|
|
|
|
|
|
Date of Referral |
|||
|
|
|
|
|
|
|
|
|
|
|
|
School |
|
|
|
|
|
|
|
Grade |
|||
|
|
|
|
|
|
|
|
|
|
||
Reason for referral (test failed or type of symptom) |
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
School Screening visual acuity |
without glasses |
with glasses |
|
|
|
|
|
|
|||
|
|
R___________ |
L ___________ |
R___________ |
L ___________ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Eye Specialist |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
Distance Visual Acuity |
without correction |
with current prescription |
with new prescription |
||||||||
|
|
R___________ |
L ___________ |
R___________ |
L ___________ |
R___________ L ___________ |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
Summary of vision problems and diagnosis |
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Recommendations |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Additional instructions for teacher |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Is further treatment necessary? |
■ Yes |
■ No |
|
I wish to see the child again. |
■ Yes |
■ No |
|||||
|
|
|
|
|
|||||||
If yes, specify |
|
|
|
If yes, when? |
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
Please return form to |
|
|
|
From |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Eye Specialist |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Address |
|
|
|
|
|
|
City
State
ZIP
Date
This form is intended for the sole use of the intended recipient and may contain privileged, sensitive, or protected health information. If you are not the intended recipient, be advised that the unauthorized use, disclosure, copying, distribution or action taken in reliance on the contents of this communication is prohibited.
HEA 4713 (Rev 6/07)