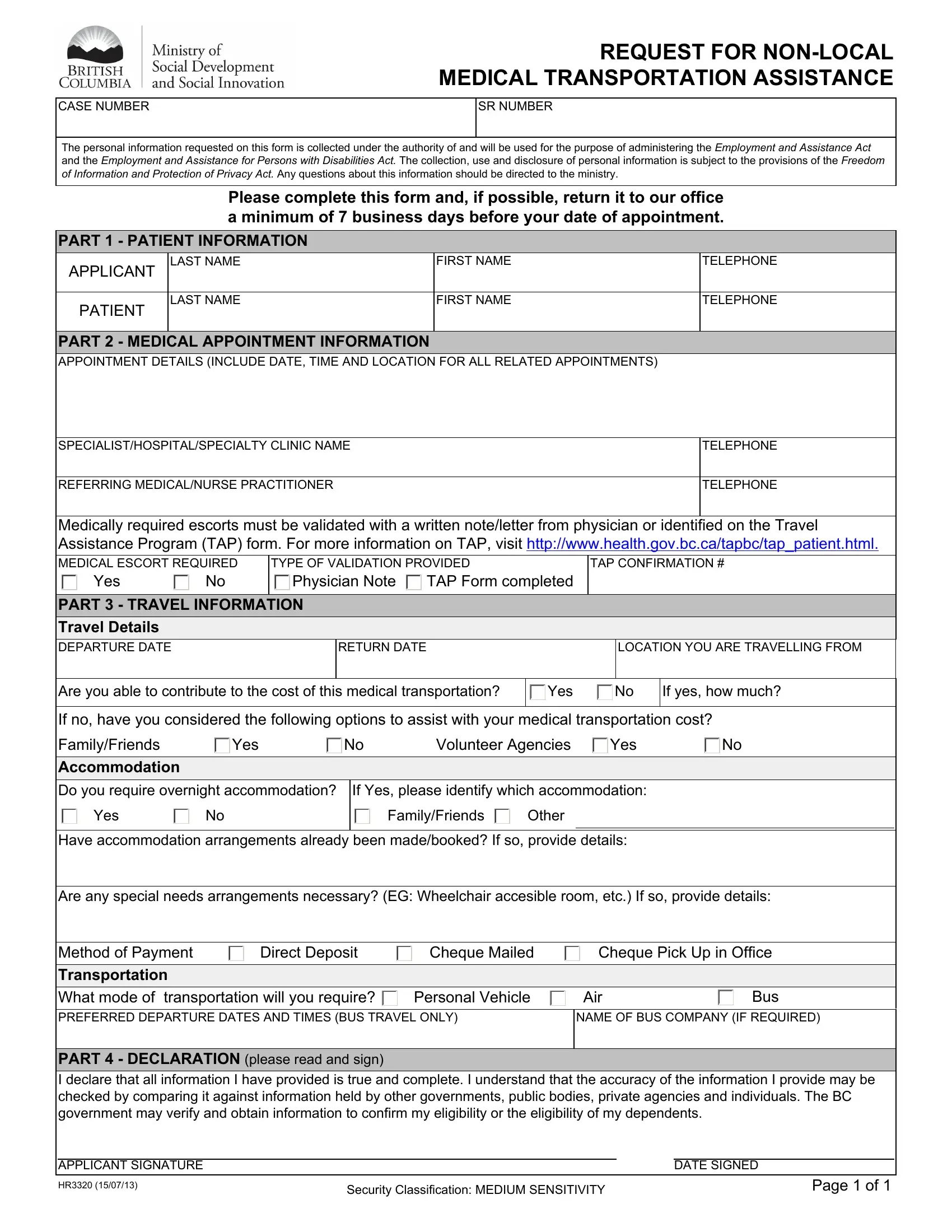
REQUEST FOR NON-LOCAL MEDICAL TRANSPORTATION ASSISTANCE
The personal information requested on this form is collected under the authority of and will be used for the purpose of administering the Employment and Assistance Act and the Employment and Assistance for Persons with Disabilities Act. The collection, use and disclosure of personal information is subject to the provisions of the Freedom of Information and Protection of Privacy Act. Any questions about this information should be directed to the ministry.
Please complete this form and, if possible, return it to our office a minimum of 7 business days before your date of appointment.
PART 1 - PATIENT INFORMATION
APPLICANT |
LAST NAME |
FIRST NAME |
TELEPHONE |
|
|
|
|
PATIENT |
LAST NAME |
FIRST NAME |
TELEPHONE |
|
|
|
|
|
|
|
PART 2 - MEDICAL APPOINTMENT INFORMATION |
|
|
APPOINTMENT DETAILS (INCLUDE DATE, TIME AND LOCATION FOR ALL RELATED APPOINTMENTS) |
|
|
|
|
SPECIALIST/HOSPITAL/SPECIALTY CLINIC NAME |
|
TELEPHONE |
|
|
|
REFERRING MEDICAL/NURSE PRACTITIONER |
|
TELEPHONE |
|
|
|
|
Medically required escorts must be validated with a written note/letter from physician or identified on the Travel Assistance Program (TAP) form. For more information on TAP, visit http://www.health.gov.bc.ca/tapbc/tap_patient.html.
MEDICAL ESCORT REQUIRED |
|
TYPE OF VALIDATION PROVIDED |
|
|
TAP CONFIRMATION # |
|
|
Yes |
No |
|
Physician Note |
TAP Form completed |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PART 3 - TRAVEL INFORMATION |
|
|
|
|
|
|
Travel Details |
|
|
|
|
|
|
|
|
|
|
|
DEPARTURE DATE |
|
|
|
RETURN DATE |
|
|
|
|
LOCATION YOU ARE TRAVELLING FROM |
|
|
|
|
|
|
|
|
|
|
|
|
Are you able to contribute to the cost of this medical transportation? |
Yes |
No |
If yes, how much? |
|
|
|
|
|
|
|
|
|
If no, have you considered the following options to assist with your medical transportation cost? |
Family/Friends |
Yes |
|
|
No |
Volunteer Agencies |
Yes |
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Accommodation |
|
|
|
|
|
|
|
|
|
|
|
Do you require overnight accommodation? |
If Yes, please identify which accommodation: |
|
|
|
Yes |
|
|
No |
|
|
|
Family/Friends |
Other |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Have accommodation arrangements already been made/booked? If so, provide details: |
|
|
Are any special needs arrangements necessary? (EG: Wheelchair accesible room, etc.) If so, provide details: |
|
|
|
|
|
Method of Payment |
|
Direct Deposit |
Cheque Mailed |
Cheque Pick Up in Office |
|
|
|
|
|
|
|
|
|
|
|
|
Transportation |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
What mode of transportation will you require? |
Personal Vehicle |
PREFERRED DEPARTURE DATES AND TIMES (BUS TRAVEL ONLY)
NAME OF BUS COMPANY (IF REQUIRED)
PART 4 - DECLARATION (please read and sign)
I declare that all information I have provided is true and complete. I understand that the accuracy of the information I provide may be checked by comparing it against information held by other governments, public bodies, private agencies and individuals. The BC government may verify and obtain information to confirm my eligibility or the eligibility of my dependents.
|
APPLICANT SIGNATURE |
|
|
DATE SIGNED |
|
|
|
|
|
|
|
|
HR3320 (15/07/13) |
Security Classification: MEDIUM SENSITIVITY |
|
Page 1 of 1 |
|
|
|
MEDICAL TRANSPORTATION
INFORMATION CHECKLIST - FOR CLIENTS
Under the BC Employment and Assistance Program, a medical transportation supplement can be provided for persons facing extraordinary travel costs associated with essential medical treatment. This supplement is available when no other financial resources are available to cover the cost.
Essential medical treatments are non-emergency, insured medical services covered by Medical Services Plan (MSP) or the Hospital Insurance Act.
The purpose of this checklist is to provide you with information on the procedures which must be followed to help determine your eligibility for a medical transportation supplement.
Local Non-Emergency Medical Transportation
If the essential medical treatment is provided locally and you require a medical transportation supplement, you must:
•Explore all options and resources (i.e. family, voluntary agencies).
•Explore all options and resources (i.e. family, voluntary agencies).
PConfirmation that the medical treatment is covered by MSP or the Hospital Insurance Act.
PNumber of appointments per week necessary for the treatment.
PExpected duration of the treatment.
PSpecify whether an escort is medically required or not required. (only eligible if accompanying a patient who is 18 years of age and under or who is incapable of travelling independently due to medical reason)
PSpecific reason why you are unable to use public transportation, if you require a taxi on an ongoing basis.
Non-Local Non-Emergency Medical Transportation
If the essential medical treatment is provided outside your home community and you require a medical transportation supplement, you must:
•Explore all options and resources (i.e. family, voluntary agencies).
•Request a written verification with the same information listed above or the Travel Assistance Program (TAP) form from your physician. TAP is a program developed by the Ministry of Health Services with participating transportation partners to provide travel assistance to eligible BC residents who are required to travel outside their home community to obtain non-emergency, physician-referred specialist medical care. For more information about the program, go to http://www.health.gov.bc.ca/msp/mtapp/tap_patient.html.
•If a TAP form is required, submit a copy of the TAP form with confirmation number.
•Please consult with your local office to determine which document (a written verification or a TAP form) is required.
•Fill out and submit a Non-Local Medical Transportation Request form (HR3320).
•If you must return to the specialist, hospital or specialty service as part of the same course of treatment, the destination specialist’s office or specialty service can complete and sign or stamp another TAP form. A new TAP form should be issued for each subsequent visit at the time the next appointment is made and a copy should be submitted to the ministry.
Your eligibility for a medical transportation supplement will be assessed once all requested information is provided and all other resources have been considered. The most affordable option will be considered.
Failure to provide the necessary information required to determine your eligibility may result in delays processing your request.
This ministry may verify the information provided and perform post audit verification to confirm that the funding was used for its intended purpose.