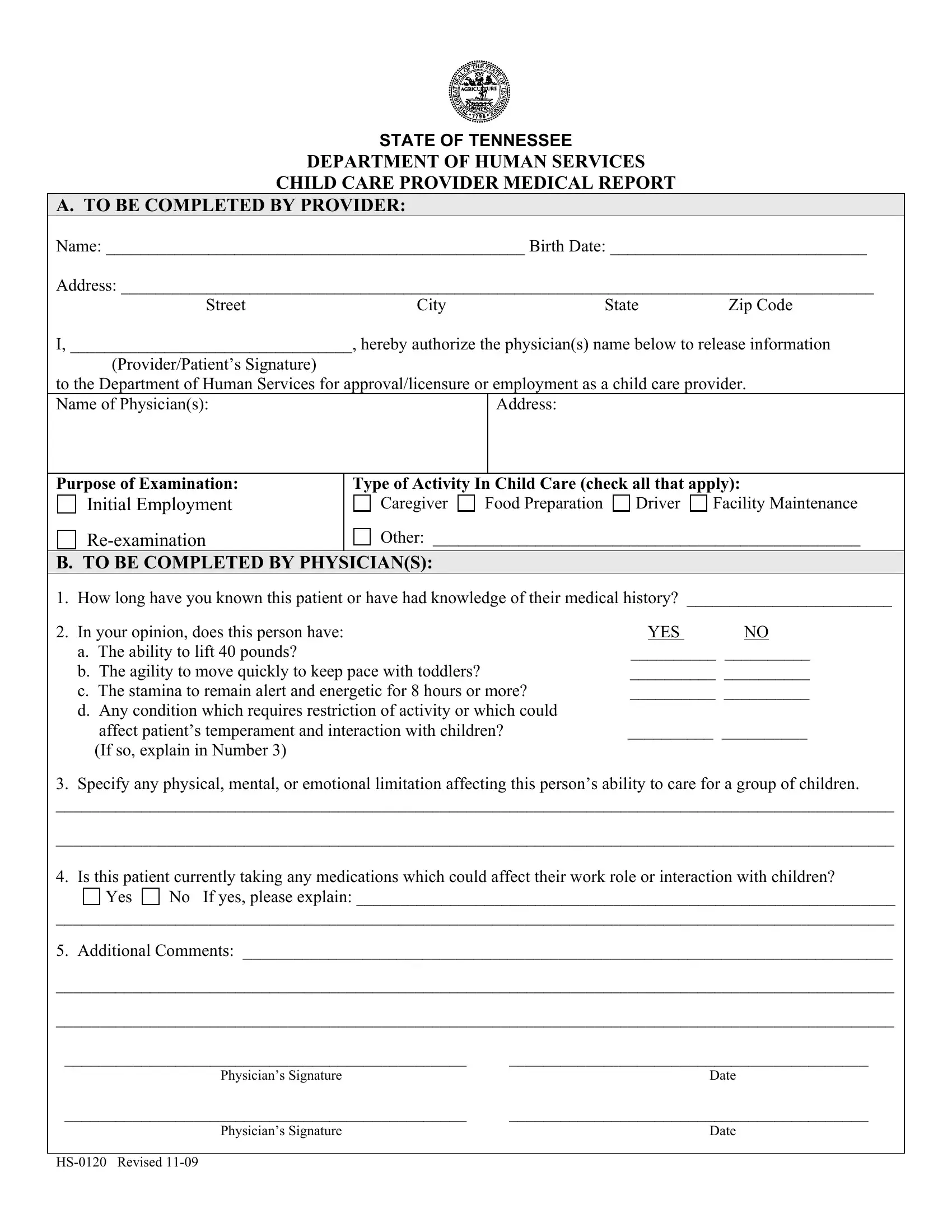
The HS-0120 form emerges as a crucial document within the Tennessee Department of Human Services, playing a central role in maintaining and ensuring the quality of child care providers. Tailored specifically towards individuals seeking approval, licensure, or employment in child care environments, this form comprises two distinct sections that cover comprehensive health-related information. The first segment calls for personal details from the provider, including authorization for physicians to share medical information pivotal for the approval process. The subsequent part, intended for completion by the physician(s), delves deep into the medical history and current health status of the applicant, evaluating their physical, mental, and emotional capability to fulfill various roles in child care settings. Questions aim to assess the provider's ability to manage physical demands typical in child care, such as lifting, agility, and stamina, and to identify any conditions that might restrict their interaction with children or influence their temperament. Physicians are also required to disclose any medications the applicant might be on that could affect their performance or interaction with children. By comprehensively vetting applicants through the HS-0120 form, the Department of Human Services strives to ensure that individuals involved in child care are not only qualified but also capable of maintaining a safe and nurturing environment for children.
| Question | Answer |
|---|---|
| Form Name | Form Hs 0120 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | tennessee hs child, tn provider medical form, tennessee child care provider medical, tennessee medical report form |
STATE OF TENNESSEE
DEPARTMENT OF HUMAN SERVICES
CHILD CARE PROVIDER MEDICAL REPORT
A. TO BE COMPLETED BY PROVIDER:
Name: _________________________________________________ Birth Date: ______________________________
Address: ________________________________________________________________________________________
StreetCityState Zip Code
I, _________________________________, hereby authorize the physician(s) name below to release information
(Provider/Patient’s Signature)
to the Department of Human Services for approval/licensure or employment as a child care provider.
Name of Physician(s): |
Address: |
|
|
Purpose of Examination:
Initial Employment
Type of Activity In Child Care (check all that apply):
Caregiver Food Preparation Driver Facility Maintenance
Other: __________________________________________________
B. TO BE COMPLETED BY PHYSICIAN(S):
1. |
How long have you known this patient or have had knowledge of their medical history? ________________________ |
||
2. |
In your opinion, does this person have: |
YES |
NO |
|
a. The ability to lift 40 pounds? |
__________ |
__________ |
|
b. The agility to move quickly to keep pace with toddlers? |
__________ |
__________ |
|
c. The stamina to remain alert and energetic for 8 hours or more? |
__________ |
__________ |
|
d. Any condition which requires restriction of activity or which could |
|
|
|
affect patient’s temperament and interaction with children? |
__________ |
__________ |
|
(If so, explain in Number 3) |
|
|
3.Specify any physical, mental, or emotional limitation affecting this person’s ability to care for a group of children.
__________________________________________________________________________________________________
__________________________________________________________________________________________________
4. Is this patient currently taking any medications which could affect their work role or interaction with children?
Yes |
No If yes, please explain: _______________________________________________________________ |
__________________________________________________________________________________________________
5.Additional Comments: ____________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
_______________________________________________ |
__________________________________________ |
Physician’s Signature |
Date |
_______________________________________________ |
__________________________________________ |
Physician’s Signature |
Date |
|
|
|